Translate this page into:
Bilateral Burow's grafts with a pulley suture: Rapid and simple reconstruction for a large defect on the vertex
Correspondence Address:
Jun Young Kim
Department of Dermatology, Kyungpook National University Hospital, 130 Dongdeok-ro, Jun-gu, Daegu, 41944
South Korea
| How to cite this article: Park JH, Lee SJ, Kim JY. Bilateral Burow's grafts with a pulley suture: Rapid and simple reconstruction for a large defect on the vertex. Indian J Dermatol Venereol Leprol 2019;85:428-430 |
Sir,
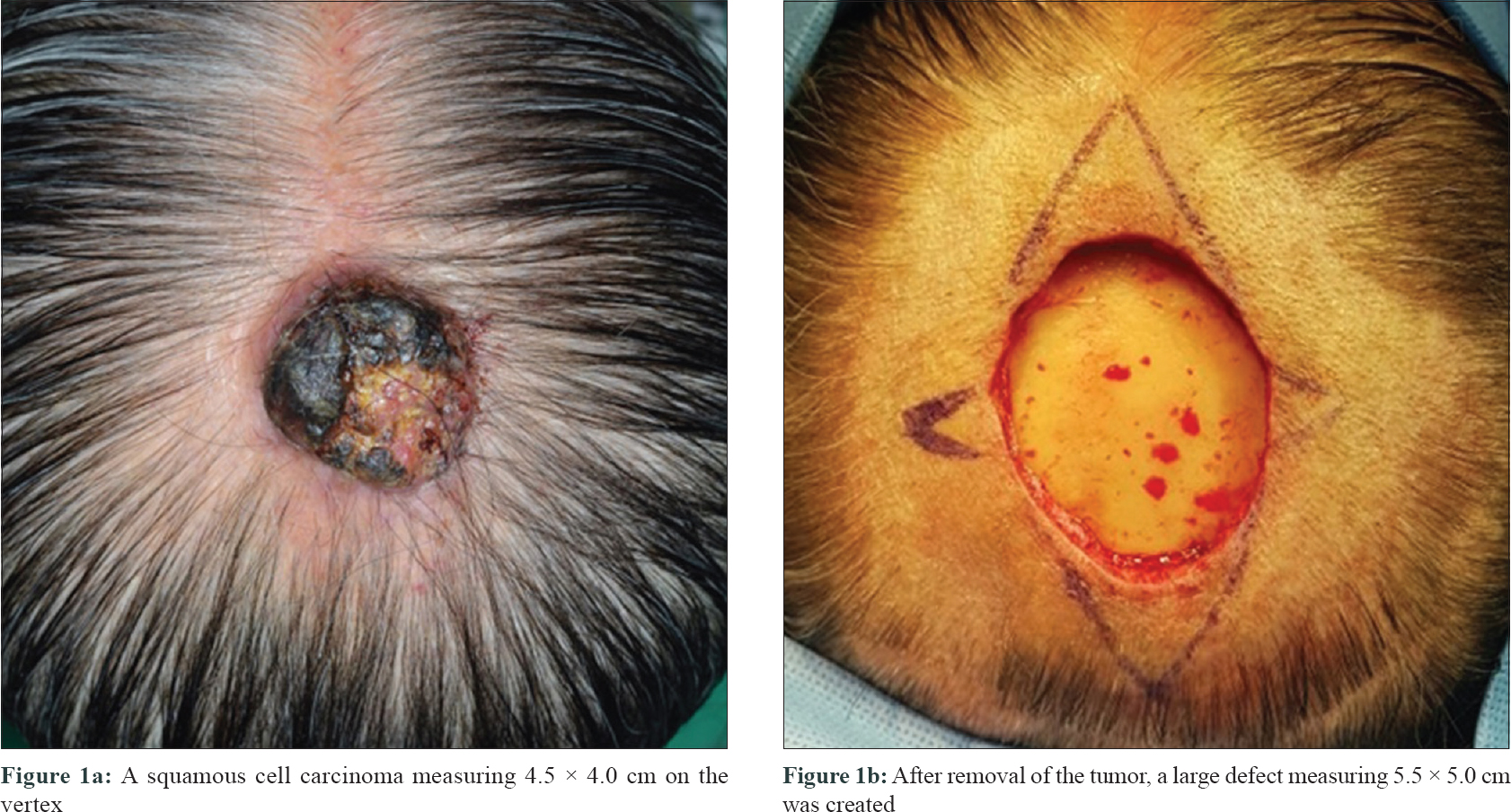
An 89-year-old woman presented with a year-old squamous cell carcinoma on her vertex of the scalp, measuring 4.5 × 4.0 cm [Figure - 1]a. Clinical lymph node metastasis was not observed on physical examination as well as on head and neck computed tomography (CT). However, the latter revealed tumor infiltration into the adjacent tissue, without any underlying skull involvement. We performed tumor extirpation with a lateral surgical margin of 5 mm and an inferior surgical margin up to the periosteum. We sent the resected specimen for pathological examination that showed clear basal resection margin without bone involvement and clear lateral resection margin of 3 mm. However, a large defect measuring 5.5 × 5.0 cm remained on her vertex [Figure - 1]b. Considering the size of the defect, cosmetic issues, and her general health, Burow's graft with a pulley suture, being the most simple and rapid procedure, was chosen. We harvested the Burow's grafts to cover the defect from both the sides. However, while closing the secondary defects we could not place dermal sutures, as her galea aponeurotica was extremely fragile. Thus, we made a pulley suture transversely across the defect to offset the tension. Since the grafts were thin enough, and to preserve the hair follicles in it, fat removal of the grafts was skipped. Finally, we successfully performed two Burow's grafts, large enough to cover the remaining defect, within 10 minutes [Figure - 2]. She received precautions of careful protection of the surgical wound and simple dressings twice a day with antibiotic ointment to prevent infection and desiccation of the wound. We removed the remaining stitches, including the pulley suture, 2 weeks after the surgery. The grafts survived well and showed good cosmetic results, without any recurrence observed at the 9-month follow-up [Figure - 3]. We initially planned to use a reconstruction option for managing the defect. It would have included a local flap, including advancement flap, O-Z flap, multiple pinwheel flap, staged purse-string suture, and full-thickness skin graft.[1],[2],[3]
 |
| Figure 1: |
 |
| Figure 2: Defect reconstructed in a simple manner with bilateral Burow's grafts with a pulley suture |
 |
| Figure 3: Surgical procedure resulted in a good cosmetic outcome, and no recurrence was observed at the 9-month follow-up |
However, the 5.5-cm-long defect was too far to advance to the surrounding scalp skin, and other local flaps or staged purse-string sutures were inappropriate because of her inelastic scalp and vulnerable galea aponeurotica. Using an ordinary full-thickness skin graft also seemed difficult, and we would have needed a long time to harvest the donor skin and close the secondary defect. Considering the size of the defect, secondary intention healing needed a long time, and a tertiary intention healing required another surgery. All the other options were infeasible. Moreover, owing to her age and poor general health, a long surgical duration would have caused complications. We needed a method that allowed rapid reconstruction of the defect. These bilateral Burow's grafts with a pulley suture could be completed within 10 minutes by skipping dermal sutures and fat removal of the grafts. Despite concerns that the grafts would be difficult to place, strong lateral tension would make troubles on the recipient site, and they would make a large patch of hair loss on the recipient site, the operation was successfully completed. The pulley suture has effectively replaced the role of dermal sutures. The pulley suture we used was a modification of vertical mattress suture, using far-near-near-far method, which is useful for reconstruction of scalp defect.[4] For her large defect on the vertex, the bilateral Burow's grafts with a pulley suture was the best choice. It required fewer additional incision lines and sutures and shorter surgical duration. Moreover, it resulted in a good cosmetic outcome because we used the tissues adjacent to the defect. Because it was performed on the vertex, it could not be seen easily when viewed from the front.[5] However, we should remember that the grafts often fail to engraft on the periosteum, and the survived grafts may appear as alopecic patch on the scalp. Several surgical options are available for the reconstruction of a large scalp defect. However, scalp tissue has limited elasticity. This factor together with cosmetic issues, including those related to the hair unit, make reconstruction of such defect always challenging.[2],[3] From this case, we may conclude that Burow's grafts with a pulley suture can also be a valuable reconstruction strategy when a rapid and simple reconstruction is needed for a large vertex defect.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given her consent for her images and other clinical information to be reported in the journal. The patient understand that name and initials will not be published and due efforts will be made to conceal identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
This study was supported financially by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (No. 2018R1C1B5085905).
Conflicts of interest
There are no conflicts of interest.
| 1. |
Nam CH, Hong SP, Kim MH, Park BC. Staged purse-string suture for repairing a large surgical defect on the scalp. J Am Acad Dermatol 2017;76:e207-8.
[Google Scholar]
|
| 2. |
Fincher EF, Gladstone HB. Dual transposition flaps for the reconstruction of large scalp defects. J Am Acad Dermatol 2009;60:985-9.
[Google Scholar]
|
| 3. |
Denewer A, Khater A, Farouk O, Hegazy M, Mosbah M, Hafez M, et al. Can we put a simplified algorithm for reconstruction of large scalp defects following tumor resection? World J Surg Oncol 2011;9:129.
[Google Scholar]
|
| 4. |
Kannan S, Mehta D, Ozog D. Scalp closures with pulley sutures reduce time and cost compared to traditional layered technique-A prospective, randomized, observer-blinded study. Dermatol Surg 2016;42:1248-55.
[Google Scholar]
|
| 5. |
Benoit A, Leach BC, Cook J. Applications of Burow's grafts in the reconstruction of mohs micrographic surgery defects. Dermatol Surg 2017;43:512-20.
[Google Scholar]
|
Fulltext Views
3,602
PDF downloads
1,768





![[Figure - 1]](#fig_ijdvl_2019_85_4_428_257740_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2019_85_4_428_257740_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2019_85_4_428_257740_f3.jpg){kind=link}