
Translate this page into:
Bilateral temporal alopecia in male androgenetic alopecia: An unusual new presentation
Corresponding author: Dr. Dingquan Yang, Department of Dermatology, China-Japan Friendship Hospital, No.2, Ying Hua Yuan East Street, Chaoyang District, Beijing, China. ydqlx@163.com
-
Received: ,
Accepted: ,
How to cite this article: Lv S, Zhang G, Wang Y, Yang D. Bilateral temporal alopecia in male androgenetic alopecia: An unusual new presentation. Indian J Dermatol Venereol Leprol. doi: 10.25259/IJDVL_936_2024
Dear Editor,
Androgenetic alopecia (AGA) is the most prevalent form of non-scarring alopecia. The prevalence of male androgenetic alopecia (MAGA) is significantly higher, ranging from 30% to 70% in Caucasian men and approximately 21.3% in Chinese men.1,2 Typically, MAGA is characterised by progressive recession of the sideburns and anterior hairline on both sides, leading to gradual thinning at the top of the head and eventual scalp exposure, while sparing the occipital region.
Here, we report a case of MAGA with an atypical presentation, identified as a special subtype termed “reverse MAGA”. In this case, the patient exhibited progressive thinning of hair in the temporal regions bilaterally with no involvement of the sideburns, anterior hairline, or the vertex of the scalp.
A 33-year-old male patient presented to our department with a 7-year history of progressive thinning of bilateral temporal hair, accompanied by an oily scalp. Dermatological examination revealed scattered sparse hair in the temporal regions bilaterally, without significant recession of the sideburns or hairline, and no notable thinning at the vertex [Figures 1a-1d]. Combined with the results of trichoscopy [Figures 1e, 1f], a preliminary diagnosis of AGA was made, while not excluding alopecia areata. The patient was initially treated with a local skin injection of 1 ml of compound betamethasone, including betamethasone dipropionate 5 mg and betamethasone disodium phosphate 2 mg, oral isotretinoin soft capsules (10 mg every other day), and topical 5% minoxidil solution (1 ml once daily). At the follow-up 3 months later, there was no significant improvement in the alopecia area, prompting a further histopathological examination to confirm the diagnosis. A local scalp biopsy performed revealed a diagnosis consistent with AGA [Figure 2a, 2b]. Subsequently, treatment was adjusted to include oral finasteride (1 mg daily), while continuing oral isotretinoin and topical 5% minoxidil. At the follow-up visit after 4 months, there was still no significant hair regrowth in the alopecia area [Figures 3a-3b]. Further immunohistochemistry testing indicated androgen receptor (AR) positivity, type I 5α-reductase (SRD5A1) negativity, and type II 5α-reductase (SRD5A2) negativity [Figure 4a-4c]. Selective hair transplantation was recommended.

- (a)Decreased density of the hair on the left temporal area, (b) on the right temporal area, (c) while vertex shows no hair thinning.
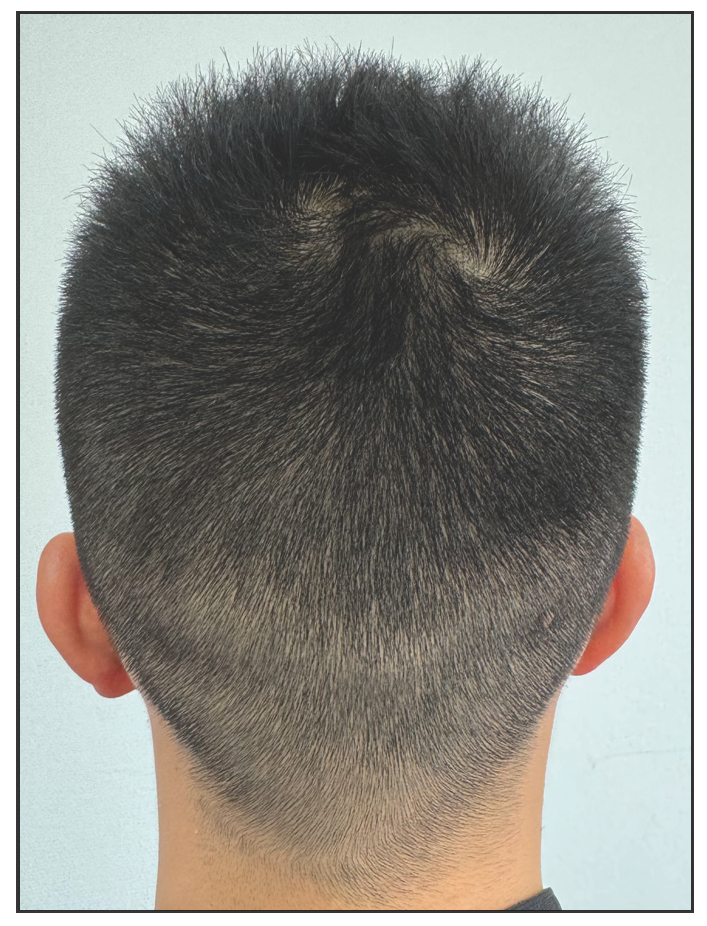
- No significant decrease in hair density over the occipital area.
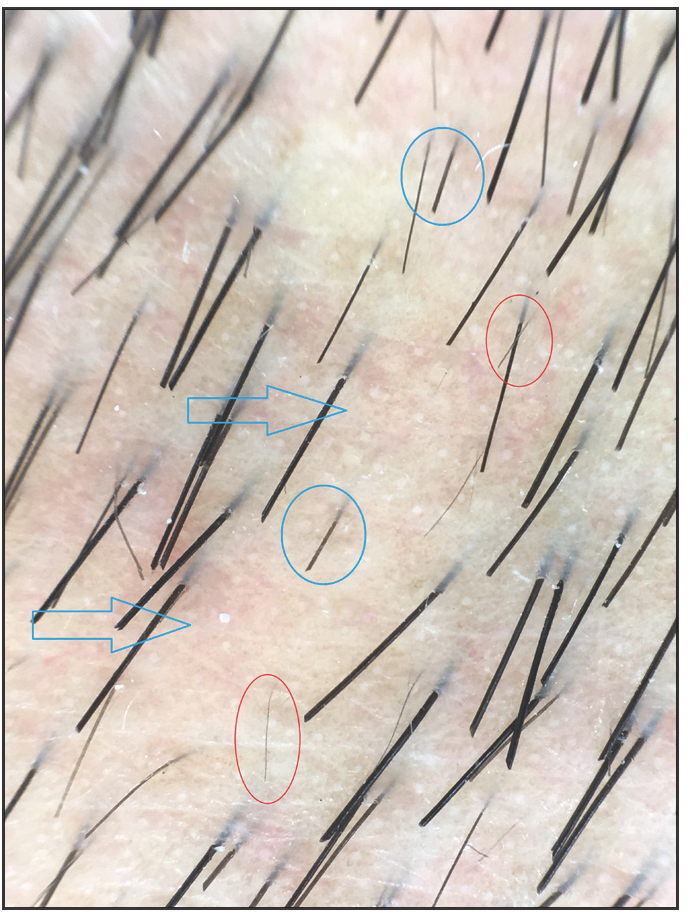
- Trichoscopic photograph (taken by fotofinder, 40× of the left side reveals partial hair loss (blue arrows), uneven hair thickness (red circles), and suspicious broken hairs (blue circles).
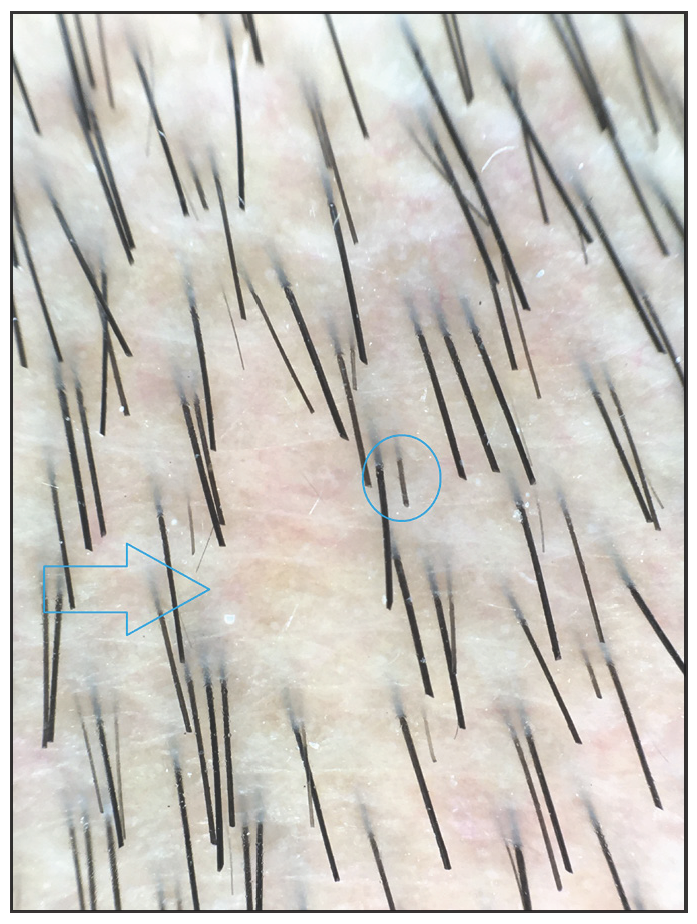
- Trichoscopic photograph (taken by fotofinder, 40× of the right side reveals partial hair loss (blue arrows) and suspicious broken hairs (blue circles).
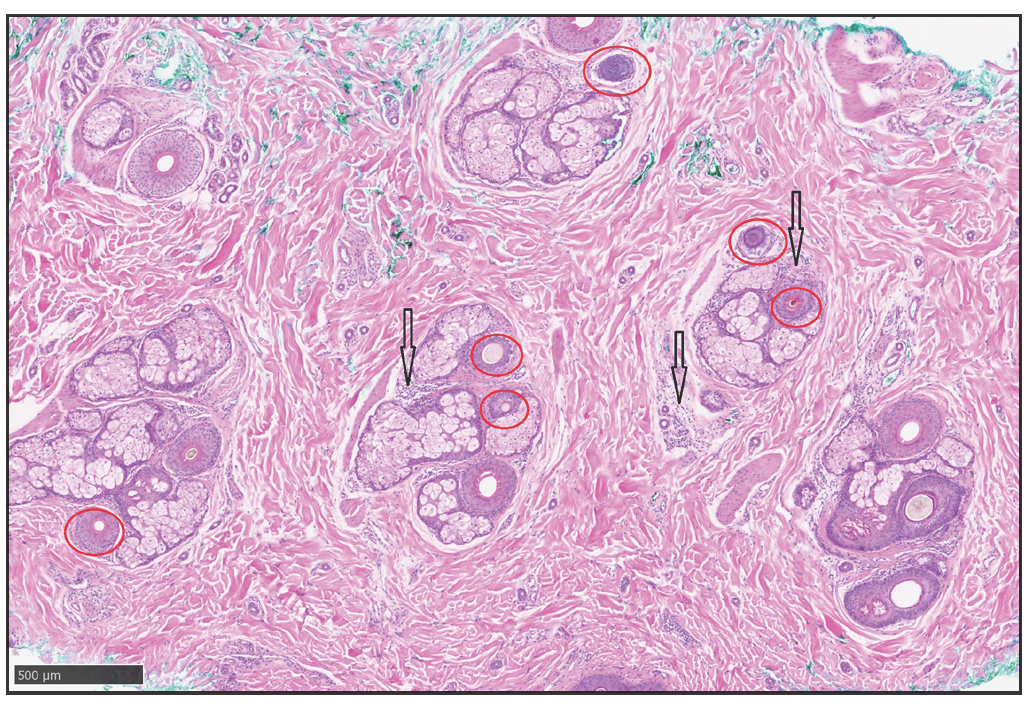
- Transverse Haematoxylin-eosin staining (200×) shows that a reduced number of hairs, miniaturised hairs (red circles), and a small amount of chronic lymphocytes infiltration around the focal hair follicles and sebaceous glands (black arrows).
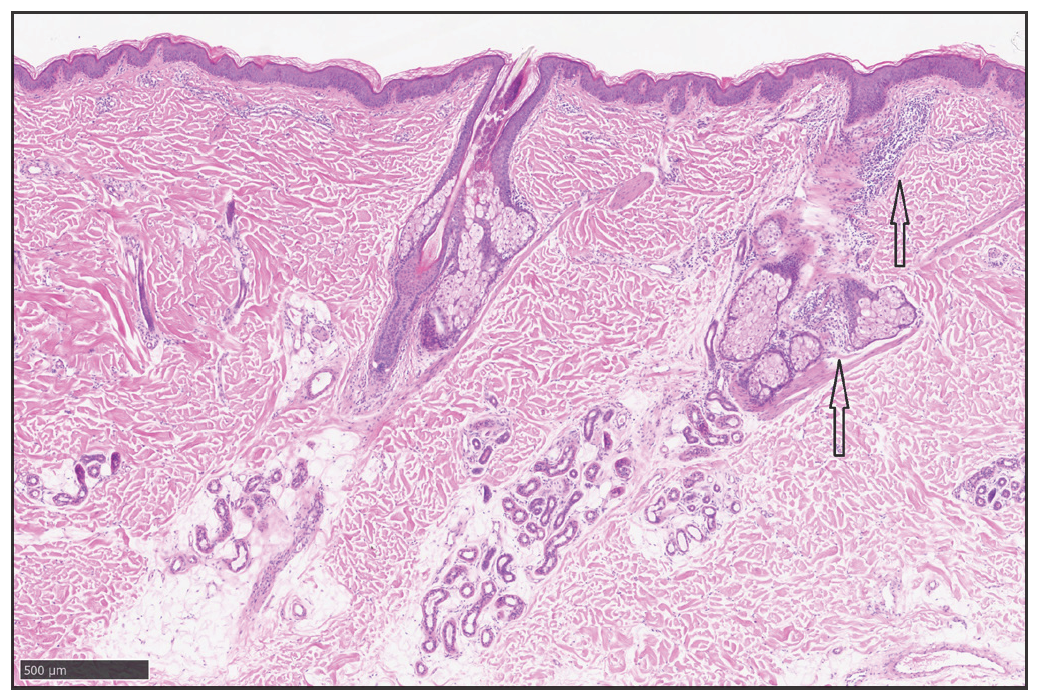
- Longitudinal Haematoxylin-eosin staining (200×) shows a small amount of chronic lymphocytes infiltration around the focal hair follicles and sebaceous glands (black arrows).

- Seven months post treatment, patient showed no significant growth on the left and right side of the scalp.
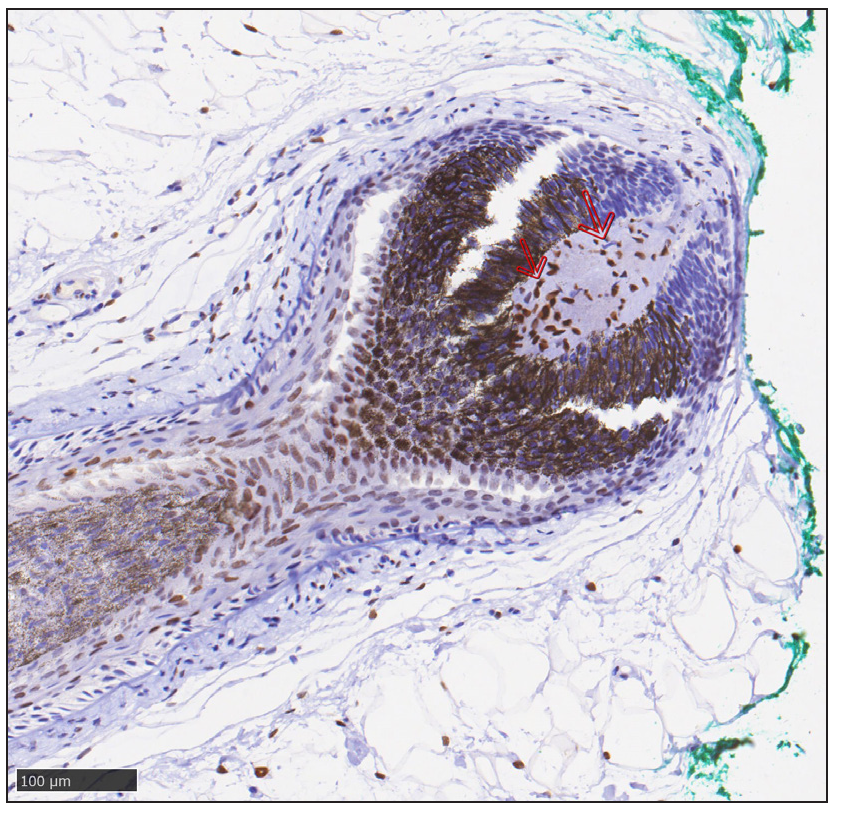
- Immunohistochemical staining shows marked expression of androgen receptor (AR) in dermal papilla cells (red arrows) at the lesion (anti-androgen receptor, ab133273, abcam).
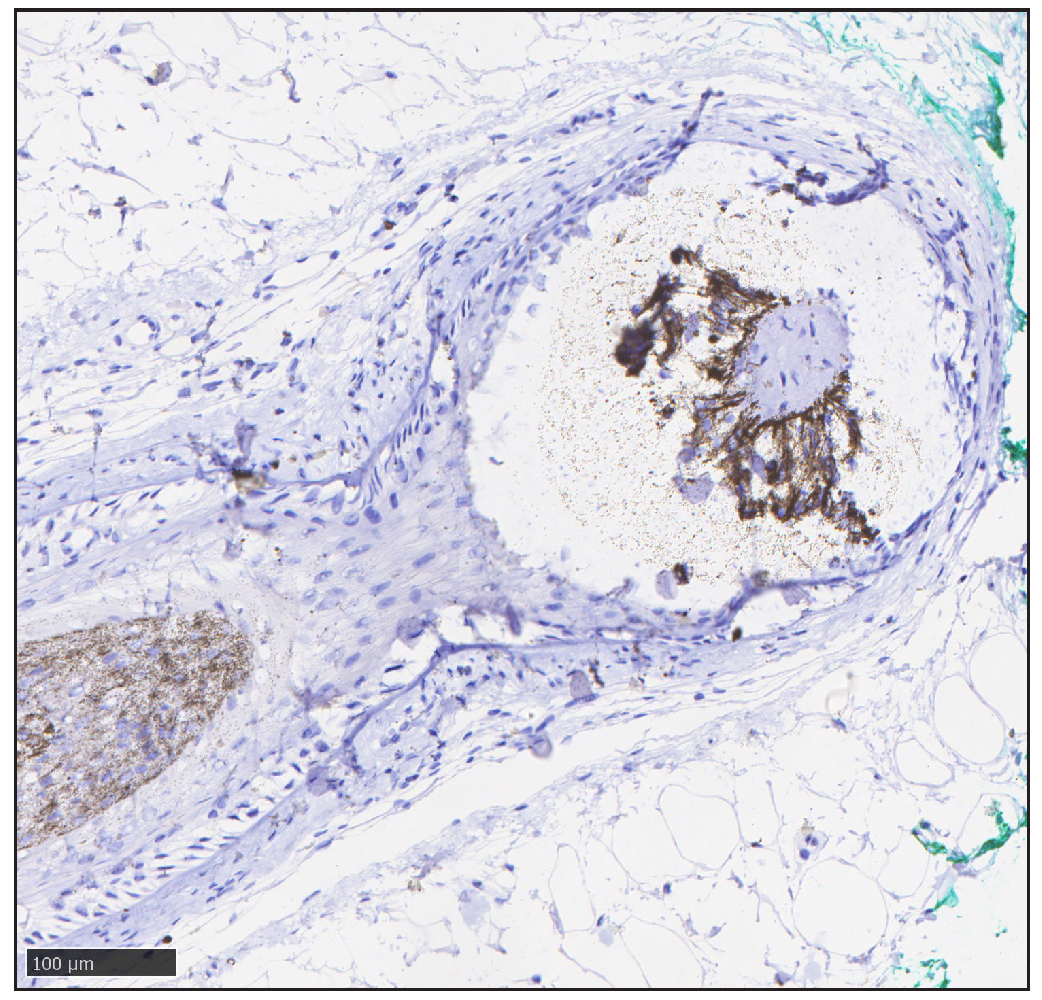
- Immunohistochemical staining shows negative type I 5α-reductase (SRD5A1) at the lesions (anti-SRD5A1, ab110123, abcam).
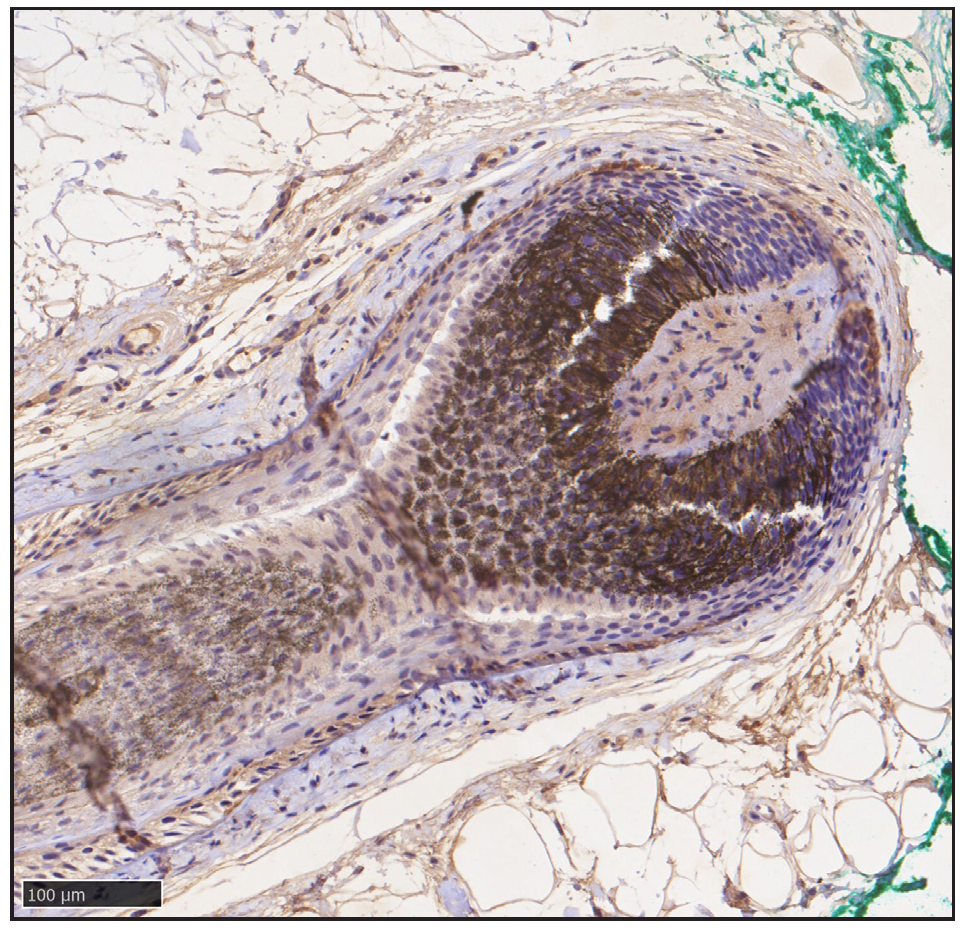
- Immunohistochemical staining shows negative type II 5α-reductase (SRD5A2) at the lesions (anti-SRD5A2, BS-6700R, Bioss).
MAGA is typically diagnosed based on patient history and clinical presentation. However, in this case, the location of hair thinning deviated from the conventional pattern. The diagnosis was confirmed through histopathological examination, underscoring the necessity of pathological diagnosis for MAGA cases with atypical clinical manifestations.
It is widely accepted that testosterone, the major circulating androgen, is converted via 5α-reductase in the cytoplasm to the more potent androgen dihydrotestosterone (DHT). DHT binds more strongly to androgen receptors (AR), thereby activating gene expression. Dermal papilla cells (DPCs) from balding scalp hair follicles contain significantly more ARs than those derived from non-balding follicles.3 In this case, immunohistochemistry revealed positive AR expression in DPCs within the temporal alopecia area, consistent with the pathological characteristics of MAGA.
Additionally, the sensitivity of hair follicles to androgens is modulated by 5α-reductase. The expression of SRD5A2 is higher in DPCs of AGA and beard follicles compared to other sites.4 However, in our patient, the clinical application of finasteride for almost 6 months was ineffective, likely due to the absence of significant SRD5A1 and SRD5A2 expression, as revealed by immunohistochemistry.
Reports on this specific type of reverse MAGA are scarce, with previous cases typically presenting in the posterior hairline and occipital region.5 This case represents the first instance of reverse MAGA affecting both temporal sides. Clinical studies on this atypical manifestation of non-pattern alopecia are limited, and existing studies indicate a differential response to traditional MAGA treatments. Therefore, further in-depth studies are necessary to systematically understand this type of MAGA and enhance the accuracy and standardisation of clinical diagnosis and treatment.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
References
- Androgenetic alopecia in China: a survey in China six provinces. J Clinical Dermatology. 2010;39:743-6.
- [Google Scholar]
- Balding hair follicle dermal papilla cells contain higher levels of androgen receptors than those from non-balding scalp. J Endocrinol. 1998;156:59-65.
- [CrossRef] [PubMed] [Google Scholar]
- 5 alpha-reductase type 2 is constitutively expressed in the dermal papilla and connective tissue sheath of the hair follicle in vivo but not during culture in vitro. J Clin Endocrinol Metab. 2001;86:2875-80.
- [CrossRef] [PubMed] [Google Scholar]
- Inverse androgenic alopecia. BMJ Case Rep. 2023;16:e254361.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]




