Translate this page into:
Blaschkoid hypermelanosis in a patient with ring 18 chromosome
Correspondence Address:
Eduardo Varas-Meis
Department of Dermatology, Complejo Asistencial Universitario de León, Altos de Navas S/N, 24080 León
Spain
| How to cite this article: Varas-Meis E, Delgado-Vicente S, Fernández-Canga P, Rodríguez Prieto M�. Blaschkoid hypermelanosis in a patient with ring 18 chromosome. Indian J Dermatol Venereol Leprol 2020;86:316-318 |
Sir,
Linear and whorled nevoid hypermelanosis is a rare sporadic pigmentary anomaly occurring in blaschkoid distribution. It has been associated with several chromosomopathies including trisomy 7, 14, 18, 20, inversion of chromosome 9 and X-chromosomal mosaicism.[1],[2],[3],[4],[5]
Ring chromosomes usually occur “de novo” due to deletion and fusion of both ends of chromosome. Ring chromosome 18 is a rare disorder characterized by severe mental retardation, microcephaly, brain and ocular malformations, hypotonia, skeletal abnormalities and immunological disorders.[6],[7]
A 4-year-old boy, after a full-term birth from eutocic delivery was diagnosed with microcephaly, psychomotor retardation, generalized hypotonia and impaired ambulation. His father had a factor V Leiden heterozygous mutation. The comparative genomic hybridization of peripheral blood demonstrated a ring 18 chromosome with 17% mosaicism. He was referred to the dermatology department due to a 3-year history of stable and asymptomatic hyperpigmented lesions which appeared within the first month of life. Upon examination, we observed a bilateral and symmetrical thoracoabdominal macular hyperpigmentation in blaschkoid distribution with midline demarcation. There were no associated hypopigmented macules or other cutaneous primary lesions [Figure - 1]. On complete examination, the patient was found to have slightly low-set ears with no other adnexal, mucosal or musculoskeletal associated abnormalities [Figure - 2].
 |
| Figure 1: Macular linear hyperpigmentation on the right thoracoabdominal area with midline demarcation |
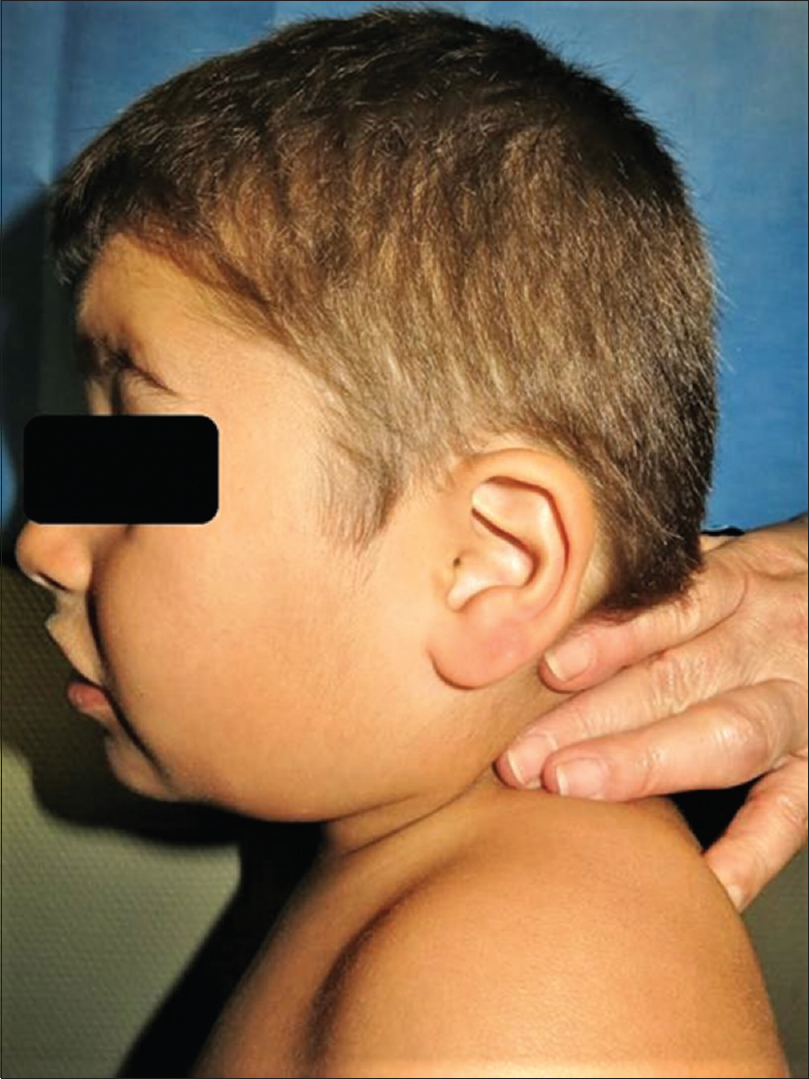 |
| Figure 2: Low-set ear |
Linear and whorled nevoid hypermelanosis, a rare sporadic pigmentary anomaly is characterized by swirls and streaks of macular hyperpigmentation in blaschkoid distribution, as described by Kalter et al. in 1988.[1] Classically, it is seen within the first 2 years of age and is distributed mainly over the trunk, neck and extremities, sparing the palms, soles and mucosa. Lesions appear without preceding inflammation, rash or injury and progress for a year or two before stabilization.[2],[3],[4],[5] No satisfactory treatments are currently available but in some patients, macules become less prominent with age. The histopathological findings reveal diffuse epidermal hyperpigmentation in the basal layer without melanocytic proliferation or pigmentary incontinence.[1],[2],[3],[4],[5]
Linear and whorled nevoid hypermelanosis has been related to the pigmentation variability in cellular mosaicisms leading to distinct population of melanocytes with different potentials of pigment production. Frequently, it has been associated with chromosomopathies including trisomy 7, 14, 18, 20, inversion of chromosome 9 and X-chromosomal mosaicism. However, its underlying pathogenesis is yet unknown. In the literature, rare cases associated with extracutaneous manifestations have been reported, mostly with cardiac defects, developmental and growth retardation or body asymmetries, among others.[2],[3],[4],[5]
The differential diagnoses include pigmentary stage of incontinentia pigmenti, hypomelanosis of Ito, early-stage linear epidermal nevus and Goltz syndrome. The clinical absence of preceding vesicular or verrucous lesions, and microscopic findings lacking pigmentary incontinence, papillomatosis, rete ridge elongation or dermal hypoplasia differentiate the linear and whorled nevoid hypermelanosis from these diseases.[3],[4] In addition, it should be remembered that early stages of incontinentia pigmenti could take place in-utero, recommending a histological examination to rule out this diagnosis.
In conclusion, we present a linear and whorled nevoid hypermelanosis in association with a mosaic ring 18 chromosome. We were unable to find any previous reports of this syndrome associated with cutaneous hypermelanosis.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given his consent for his images and other clinical information to be reported in the journal. The patient understands that name and initials will not be published and due efforts will be made to conceal identity but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Kalter DC, Griffiths WA, Atherton DJ. Linear and whorled nevoid hypermelanosis. J Am Acad Dermatol 1988;19:1037-44.
[Google Scholar]
|
| 2. |
Di Lernia V. Linear and whorled hypermelanosis. Pediatr Dermatol 2007;24:205-10.
[Google Scholar]
|
| 3. |
Ito T, Yoshida Y, Goto H, Furue M, Yamamoto O. Linear and whorled nevoid hypermelanosis with tetralogy of fallot. Indian J Dermatol 2015;60:325.
[Google Scholar]
|
| 4. |
Hong SP, Ahn SY, Lee WS. Linear and whorled nevoid hypermelanosis: Unique clinical presentations and their possible association with chromosomal abnormality inv (9). Arch Dermatol 2008;144:415-6.
[Google Scholar]
|
| 5. |
Komine M, Hino M, Shiina M, Kanazawa I, Soma Y, Tamaki K. Linear and whorled naevoid hypermelanosis: A case with systemic involvement and trisomy 18 mosaicism. Br J Dermatol 2002;146:500-2.
[Google Scholar]
|
| 6. |
Lo-Castro A, El-Malhany N, Galasso C, Verrotti A, Nardone AM, Postorivo D, et al. De novo mosaic ring chromosome 18 in a child with mental retardation, epilepsy and immunological problems. Eur J Med Genet 2011;54:329-32.
[Google Scholar]
|
| 7. |
Heydari S, Hassanzadeh F, Hassanzadeh Nazarabadi M. Ring chromosome 18: A case report. Int J Mol Cell Med 2014;3:287-9.
[Google Scholar]
|
Fulltext Views
4,232
PDF downloads
2,276





![[Figure - 1]](#fig_ijdvl_2020_86_3_316_281360_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2020_86_3_316_281360_f2.jpg){kind=link}