Translate this page into:
Bullous pemphigoid induced by topical PUVASOL
Correspondence Address:
Najeeba Riyaz
Department of Dermatology and Venereology, Government Medical College, Kozhikode - 673 008, Kerala
India
| How to cite this article: Riyaz N, Nasir N, Bindu V, Sasidharanpillai S. Bullous pemphigoid induced by topical PUVASOL. Indian J Dermatol Venereol Leprol 2014;80:363-364 |
Sir,
Vitiligo is a multifactorial polygenic disorder characterized by the destruction of epidermal melanocytes. Other autoimmune disorders like alopecia areata and thyroid disorders are well known to coexist with vitiligo. Bullous pemphigoid has been reported following thermal burns, localized trauma, UV light and radiotherapy and at sites of skin grafting. [1],[2] Drugs like beta-lactams, macrolides, co-trimoxazole, nonsteroidal anti-inflammatory agents and systemic psoralens, followed by exposure to ultraviolet rays (PUVA) [3] or sunlight (PUVASOL) [4] may also precipitate this disease.
We report a 45-year-old lady who developed bullous pemphigoid following topical PUVASOL application for vitiligo. She presented with blisters over her trunk and limbs which had developed over 10 days. She also had vitiligo for the past two years. Her vitiligo was initially treated with topical corticosteroids and five months earlier, she had been started on topical 8-methoxy psoralen followed by sun exposure for 15 minutes. While on this therapy, she developed itchy, red, raised lesions, initially over vitiligo patches on her lower limbs and subsequently on vitiligo patches on her trunk and upper limbs as well as on normal skin. Within a span of four to six days, blisters appeared over all the red raised areas, some of which broke down to form erosions that healed gradually. At this point, she came to our referral hospital. Her medical history was otherwise non-contributory. Clinical examination revealed multiple erythematous plaques varying in size from 2 × 3 cm to 6 × 5 cm over the ear-lobes, neck, chest, areola, axilla, back, upper and lower limbs involving both vitiliginous and non vitiliginous areas. The erythematous plaques were studded with numerous discrete and grouped vesicles and bullae and a few erosions [Figure - 1] and [Figure - 2]. Both Nikolsky and bulla spread signs were absent. Systemic examination detected no abnormality. A Tzanck smear revealed plenty of eosinophils and a few lymphocytes. Complete hemogram, peripheral smear analysis, chest radiography, ultrasonogram of abdomen and pelvis were within normal limits. The differential diagnoses considered were bullous pemphigoid and linear IgA bullous dermatosis. Biopsy of a fresh vesicle [Figure - 3]a showed a subepidermal blister with eosinophils and a few lymphocytes, suggestive of bullous pemphigoid. Immunoflourescence was confirmatory, showing linear deposits of IgG and C3 along the basement membrane zone [Figure - 3]b and the salt split preparation showed antigens on the roof of the blister. The patient was started on prednisolone, initially in a dose of 1 mg/kg/day, along with dapsone 100 mg/day, antihistamines and a course of antibiotics. Topical PUVASOL was withheld during the hospital stay. The patient responded well and was discharged on this treatment. At follow up one month later, the patient was asymptomatic and was taking daily doses of prednisolone, 20 mg and dapsone, 100 mg. At this point, topical PUVASOL was reintroduced, as there was no documented literature linking it to bullous pemphigoid, although there are reports of systemic PUVA therapy precipitating bullous pemphigoid. Within a week of restarting topical PUVASOL, there was a relapse of bullous pemphigoid lesions all over the body on vitiliginous and non-vitiliginous skin. Topical PUVASOL was withdrawn and the daily dose of prednisolone was stepped up to 30 mg which brought about remission of the disease within 2-3 weeks. When evaluated 6 months after the last admission, the patient was free of pemphigoid lesions and she had stopped systemic steroid therapy. Her vitiligo improved and became stable while on systemic steroids, and she subsequently refused further treatment for vitiligo. She was still on dapsone 100 mg daily which we planned to taper off more slowly.
 |
| Figure 1: Vesicles and erosions over the vitiligo patches as well as normal skin on the legs |
 |
| Figure 2: Vesicles and erosions over the vitiligo patches as well as normal skin on the trunk |
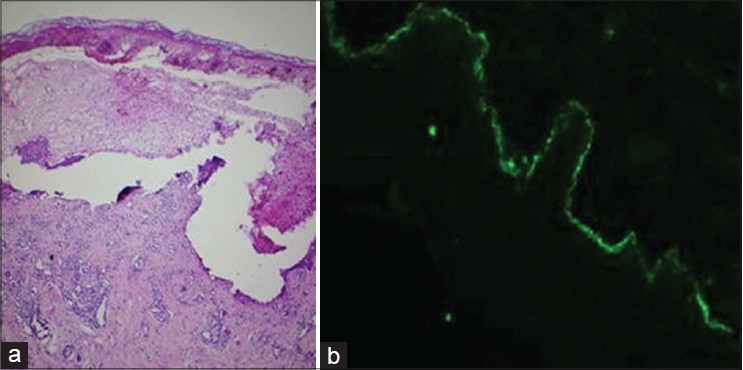 |
| Figure 3: (a) Skin biopsy from the vesicle showing a sub-epidermal cleft (H and E, ×100). (b) Direct immunofl ourescence delineating linear deposits of IgG and C3 along the basement membrane zone |
In our patient, vitiligo preceded bullous pemphigoid by almost 2 years. It was interesting to note that bullous pemphigoid developed within 5 months of starting topical PUVASOL and the initial lesions appeared over the depigmented patches. Initiation of the disease while on topical PUVASOL, remission on stopping it and relapse on re-introduction of topical PUVASOL suggests that the topical therapy might have precipitated bullous pemphigoid. The exact pathogenesis of PUVA in the induction of bullous pemphigoid is unknown. It is thought that intense UV light therapy may induce alteration of the normal human basement membrane zone thus exposing antigens to which the host responds with autoantibodies [5] resulting in the development of sub-epidermal blisters.
Kumar et al.[4] reported a case of bullous pemphigoid following systemic PUVASOL for psoriasis. Though there are reports of systemic PUVA precipitating bullous pemphigoid, we were unable to find other published report of topical PUVA precipitating a vesiculobullous disorder.
| 1. |
Venning V, Wojnarowska F. Induced bullous pemphigoid. Br J Dermatol 1995;132:831-2.
[Google Scholar]
|
| 2. |
Sacher C, Konig C, Scharffetter-Kochanek K, Krieg T, Hunzelmann N. Bullous pemphigoid in a patient treated with UVA-1 phototherapy for disseminated morphea. Dermatology 2001;202:54-7.
[Google Scholar]
|
| 3. |
Perl S, Rappersberger K, Fodinger D, Anegg B, Honigsmann H, Ortel B. Bullous pemphigoid induced by PUVA therapy. Dermatology 1996;193:245-7.
[Google Scholar]
|
| 4. |
Kumar P, Jain RK, Sharma PK, Kar HK. PUVASOL induced bullous pemphigoid in a case of psoriasis. J Clin Diagn Res 2007;1:537-9.
[Google Scholar]
|
| 5. |
Robinson JK, Baughman RD, Provost TT. Bullous pemphigoid induced by PUVA therapy. Is this the aetiology of the acral bullae produced during PUVA treatment? Brit J Dermatol 1978;99:709-13.
[Google Scholar]
|
Fulltext Views
1,992
PDF downloads
1,078





![[Figure - 1]](#fig_ijdvl_2014_80_4_363_136936_u1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2014_80_4_363_136936_u2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2014_80_4_363_136936_u3.jpg){kind=link}