Translate this page into:
Calcipotriol and adapalene therapy for disseminated superficial actinic porokeratosis
Correspondence Address:
Yoshitaka Nakamura
Department of Dermatology, Yamaguchi University Graduate School of Medicine, 1-1-1 Minami-Kogushi, Ube, Yamaguchi - 755-8505
Japan
| How to cite this article: Nakamura Y, Yamaguchi M, Nakamura A, Muto M. Calcipotriol and adapalene therapy for disseminated superficial actinic porokeratosis. Indian J Dermatol Venereol Leprol 2014;80:373-374 |
Sir,
Disseminated superficial actinic porokeratosis (DSAP) is a chronic disorder of keratinization characterized by numerous papules and plaques distributed on sun-exposed sites. Although various therapeutic options are available, an ideal and standardized treatment protocol for DSAP is lacking. Here, we report a case of DSAP in an otherwise healthy 63-year-old Japanese man who was successfully treated with calcipotriol and adapalene.
A 63-year-old Japanese male carpenter was referred to our department with a 10-year history of multiple, brown, occasionally itchy lesions over the extremities in a photodistributed pattern. The lesions, diagnosed as eczema by a local doctor, had not responded to topical corticosteroids. There was worsening after sun exposure and during summer and the patient used to wear long-sleeved clothes to prevent exacerbation. He was otherwise healthy and denied any history of immunosuppression, radiation therapy, or arsenic intake. His family history was negative for DSAP and other relevant dermatological diseases.
On physical examination, multiple, red-brown, annular keratotic lesions measuring up to 1 cm in diameter were symmetrically distributed on sun-exposed areas of the extremities [Figure - 1]a. Some scaly plaques were observed on the face but the trunk was not involved. Close inspection revealed that individual lesions had central atrophy and an elevated hyperkeratotic ridge. Dermoscopic examination revealed open pores with plugs and a whitish peripheral rim [Figure - 1]b. The results of routine laboratory investigations were within normal limits. A punch biopsy taken from the keratotic border of a lesion on the right lower arm revealed a characteristic keratin-filled invagination with a cornoid lamella and absence of granular layer beneath the cornoid lamella [Figure - 1]c. A diagnosis of disseminated superficial actinic porokeratosis (DSAP) was made and topical treatment with 0.005% calcipotriol ointment twice daily was started. However, after the first 3 months, only a slight improvement was observed and treatment was changed to calcipotriol once daily in the morning and topical adapalene (0.1%) gel every night. After 3 months of treatment with both calcipotriol and adapalene, the skin lesions improved substantially leaving only slight hyperpigmentation [Figure - 1]d. The treatment was well tolerated without significant adverse effects and no recurrence was seen after reducing the frequency of topical application to every other day.
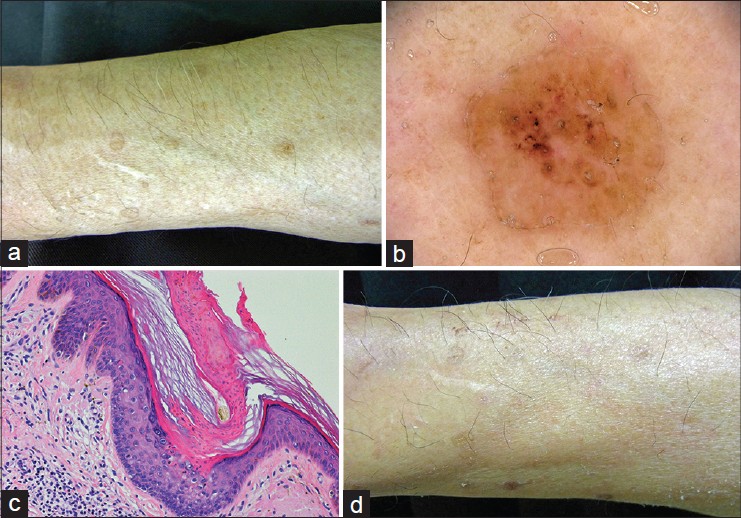 |
| Figure 1: (a) Pretreatment. Multiple red-brown, annular keratotic macules on the right lower arm. (b) Dermoscopic examination reveals open pores with plugs and a whitish peripheral rim. (c) Histopathological examination of a punch biopsy taken from the keratotic border reveals a characteristic keratin-filled invagination with cornoid lamella and absence of a granular layer beneath the cornoid lamella (H and E, ×200). (d) Clinical findings after 3 months of combination therapy. The skin lesions have improved, leaving only slight hyperpigmentation |
DSAP was first described by Chernosky and Freeman. [1] Since then, various treatment options for this condition including topical diclofenac, vitamin D 3 analogs, 5-fluorouracil, retinoids, 5% imiquimod, photodynamic therapy, carbon dioxide laser and oral retinoids have been reported with varying degrees of success. [2] However, reports of DSAP treated with vitamin D 3 analogs are rare. [3] Vitamin D 3 analogs are thought to induce the transcription of genes necessary for keratinocyte differentiation such as transglutaminase and involucrin. They may also inhibit keratinocyte proliferation by inducing sphingomyelin hydrolysis and modulation of protein kinase C activity. Harrison and Stollery reported a 50-75% improvement of DSAP lesions treated with daily topical calcipotriol for 6-8 weeks; [4] however, only a limited effect was observed in our patient on treatment with topical calcipotriol alone.
There are several reports of the successful use of topical retinoids especially tretinoin for the treatment of porokeratosis. [5] The third-generation topical retinoid, adapalene has also been used effectively for various keratotic skin diseases and has the advantage of having lesser adverse effects. In addition to its strong anti-inflammatory activity, it also acts as a modulator of keratinization and cellular differentiation. Its activity is mediated through selective binding to the nuclear retinoic acid receptor which is able to normalize differentiation of follicular epithelial cells. We believe that calcipotriol and adapalene combination therapy normalizes keratinocyte differentiation and inhibits keratinocyte proliferation more effectively through two different pathways. As demonstrated by its clinical efficacy and lack of significant adverse effects in our single patient, combination topical therapy with calcipotriol and adapalene may represent a useful option for DSAP. Further studies on a larger population of patients are necessary to confirm its therapeutic benefit.
| 1. |
Chernosky ME, Freeman RG. Disseminated superficial actinic porokeratosis (DSAP). Arch Dermatol 1967;96:611-24.
[Google Scholar]
|
| 2. |
Skupsky H, Skupsky J, Goldenberg G. Disseminated superficial actinic porokeratosis: A treatment review. J Dermatolog Treat 2012;23:52-6.
[Google Scholar]
|
| 3. |
Bakardzhiev I, Kavaklieva S, Pehlivanov G. Successful treatment of disseminated superficial actinic porokeratosis with calcipotriol. Int J Dermatol 2012;51:1139-42.
[Google Scholar]
|
| 4. |
Harrison PV, Stollery N. Disseminated superficial actinic porokeratosis responding to calcipotriol. Clin Exp Dermatol 1994;19:95.
[Google Scholar]
|
| 5. |
Agrawal SK, Gandhi V, Madan V, Bhattacharya SN. Topical tretinoin in Indian male with zosteriform porokeratosis. Int J Dermatol 2003;42:919-20.
[Google Scholar]
|
Fulltext Views
5,425
PDF downloads
1,926





![[Figure - 1]](#fig_ijdvl_2014_80_4_373_136981_u1.jpg){kind=link}