Translate this page into:
Clinical and epidemiological profile of sexually transmitted infections in a tertiary care centre in Kerala: A 1-year observational study
2 Department of Community Medicine, Government Medical College, Kozhikode, Kerala, India
Correspondence Address:
Manikoth P Binitha
Haritha, Post Beypore, Kozhikode, Kerala - 673 015
India
| How to cite this article: Jayasree P, Binitha MP, Najeeba R, Biju G. Clinical and epidemiological profile of sexually transmitted infections in a tertiary care centre in Kerala: A 1-year observational study. Indian J Dermatol Venereol Leprol 2015;81:500-503 |
Sir,
Epidemiological studies that assess the various factors responsible for sexually transmitted infections in the local population are useful for successful control efforts. This cross-sectional descriptive study was done to analyze the demographic and epidemiological features of patients attending the sexually transmitted infections clinic at our tertiary care centre. In addition, the clinical pattern of the various sexually transmitted infections and their association with human immunodeficiency virus infection was also studied.
All the patients diagnosed with a new-onset sexually transmitted infection (excluding isolated human immunodeficiency virus infection) in the department of dermatology and venereology, Government Medical College, Kozhikode, from March 2012 to March 2013 were included in the study. Institutional ethics committee approval and written informed consent from all patients were obtained. Detailed socio-economic and behavioral data were collected in a pre-designed format. A complete diagnostic evaluation was performed, including clinical examination, routine and special investigations. The modified Kuppuswami classification was used to calculate the socio-economic status by combining education, occupation and monthly family income. [1] Statistical analysis was performed using statistical package for the social sciences (SPSS) 17.0 software. Calculation of frequency tables and plotting of graphs was done from the master chart. Between groups analysis was done by Pearson chi-square tests, odds ratio and linear by linear association.
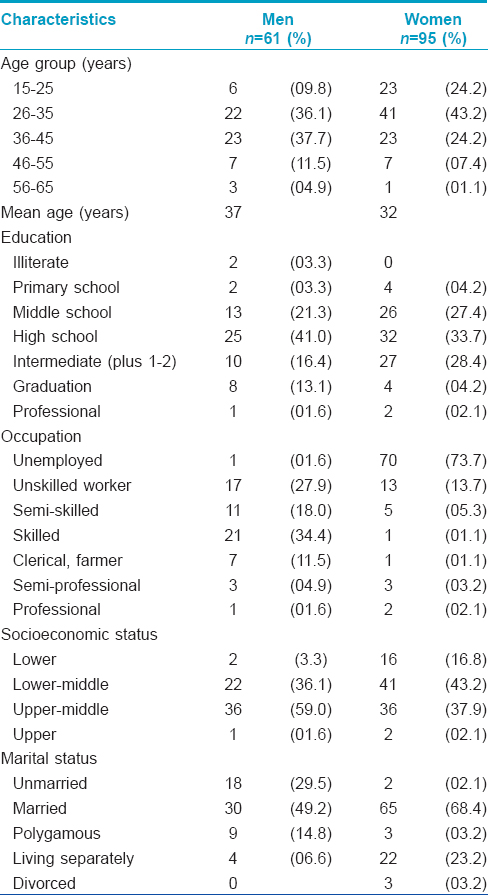
Of 156 new patients who presented during the study period, 95 (60.9%) were women and 61 (39.1%) were men. Fifty eight percent of patients were from the district where the hospital was located, 36.8% were referred from other districts another 5.2% were migrant laborers from other states. Almost half the patients (46% comprising of 23% each equally of men and women) had an upper middle socio-economic status.
Among the male patients, 49% were married, 30% unmarried, 15% polygamous and 7% were living separately from their wives. Of the female patients 68% were married, 23% living separately, 3% had multiple marital partners, 3% were divorcees and 2% were unmarried [Table - 1]. There was a statistically significant difference in the marital status of men and women (P = 0.001).
The mean age of coital debut was 20.3 years. It was significantly lower in women (less than 18 years in 37.8%) when compared with men (less than 18 years in 0.04%; P < 0.001). A higher socio-economic status was associated with an older age of coital debut in women, and conversely, a lower age of coital debut in the case of men [Figure - 1] and [Figure - 2].
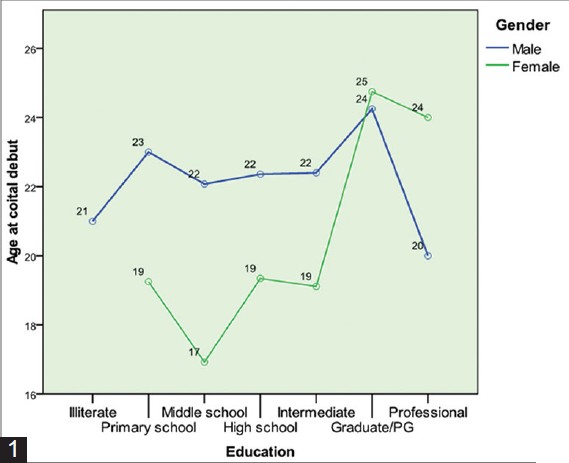 |
| Figure 1: Correlation between age of coital debut, education and socioeconomic status |
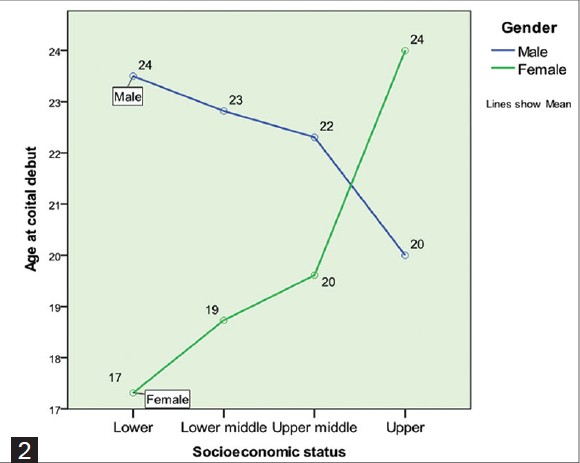 |
| Figure 2: Correlation between age of coital debut, education and socioeconomic status |
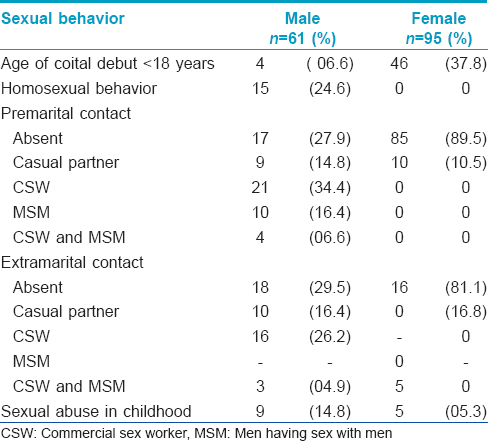
The male partners of 85 (89.5%) out of the 95 women in the study reported extramarital contact with commercial sex workers or casual partners. Almost all these extramarital contacts (97%), in turn, were married, thus forming a significant bridge population. Polygamy was reported by 14.8% of the male partners of the women, and 6.6% reported bisexual behavior with both commercial sex workers and men who have sex with men. Male migrants who were away from their spouses formed 39% of this population with sexual concurrency (more than one partner during a relationship).
Among the 61 men in the study, 15 (27%) reported homosexual activity (4% were active, 9% passive, 14% both active and passive). Three of them (two of whom were seropositive for human immunodeficiency virus) reported commercial sex activity. Two women in the study group were also commercial sex workers. However, there were no homosexuals among the women in the study group.
Only 38% of the men were circumcised. Occasional use of condoms was reported by 16% of men. None of the men reported consistent or correct use of condoms. Awareness about condoms for protection against sexually transmitted infections was low. If used, they were mainly used with commercial sex workers. Many participants felt that marital and homosexual sex were safe.
A history of sexual abuse in childhood was present in 9% of patients, 9 men and 5 women. The perpetrator was a relative in most cases. Among these, 66% of the male victims reported homosexual activity in adulthood. A statistically significant association was found between sexual abuse in childhood and smoking (P = 0.004), alcohol and injectable drug use (P < 0.001) in adulthood. [Table - 2] shows the pattern of sexual behavior of the study group.
[Table - 3] shows the prevalence of sexually transmitted infections in the study group. Genital herpes and condyloma acuminata were the two most common infections. Among the 53 patients with genital herpes, 49% presented with primary first episode, 9% with non-primary first episode and 42% with recurrent episodes. Of 11 cases of syphilis, 9 (81.8%) were seen in men. There was a single case each of primary and secondary syphilis, both in human immunodeficiency virus infection seropositive men. Syphilis of unknown duration was detected in nine patients.
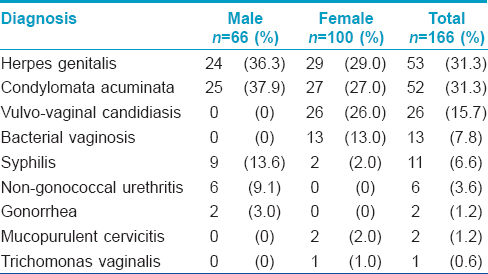
Twelve (7.7%) patients had more than one sexually transmitted infection. There were four cases of co-infection of genital herpes and vulvo-vaginal candidiasis, four cases of genital herpes and non-gonococcal urethritis, two cases of condyloma acuminata and non-gonococcal urethritis, and one case each of syphilis of unknown duration associated with genital herpes, and condyloma acuminata associated with vulvo-vaginal candidiasis.
The prevalence of extramarital contact was much higher in patients with multiple sexually transmitted infections as compared with patients with a single infection (73% vs. 29%; P = 0.0038). On calculating linear by linear association, casual partner contact (36%) was more common than commercial sex worker contact (27%) in these patients.
There were 27 (17%) patients with a total of 29 prevalent sexually transmitted infections, who were seropositive for human immunodeficiency virus. Their clinical stages were stage 2 (40%), stage 3 (37%), stage 1 and 4 (6.5% each). Though herpes genitalis was the most common condition in these patients, seropositivity was greatest in patients with syphilis (36% vs. 30% in patients with herpes genitalis). A history of intravenous drug abuse was present in 27% of these patients compared with 1% of the seronegative patients; this difference was significant (P < 0.001) [Figure - 3]. Contact tracing was possible in half the cases (50%). Partner referral was more effective (97%) in the case of marital contacts.
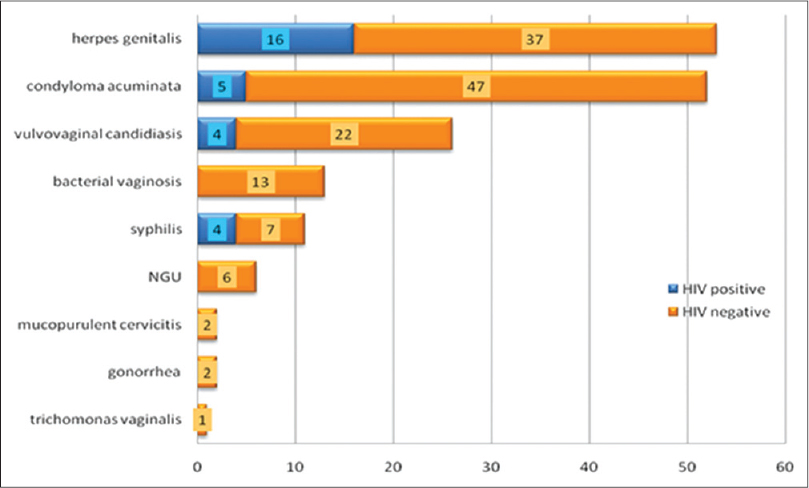 |
| Figure 3: Comparison of infections in HIV positive and negative patients. HIV: Human immunodeficiency virus, NGU: Nongonococcal urethritis |
In our study, almost two-thirds of the study population were women with a good education and socio-economic status. Studies have shown that in regions where women have an inferior educational and social status, there is very low attendance in the sexually transmitted infections clinics, as in the study done in Kuwait where women constituted only 0.025% of the patients. [2] Similar findings have been reported from India and Pakistan. [3],[4]
While almost two-thirds of the study population were married, a significant proportion of this group was not cohabiting, mostly due to work-related emigration. This separated status was a significant association because Kerala has a large expatriate male population. The husband had a history of extramarital contact in more than three-quarters of the women in the study. Male migrants are more likely to have multiple commercial and non-commercial, heterosexual and homosexual sex partners, often without condom protection, as well as injectable drug use. [5]
The high prevalence of genital herpes and condyloma acuminata in our study is in concordance with the worldwide trend indicating an increase in viral infections especially genital herpes and a decline in bacterial sexually transmitted infections, along with a resurgence of syphilis. In this study, syphilis was most often associated with the human immunodeficiency virus seropositivity indicating that it remains an important portal of entry for the virus.
In conclusion, individuals with sexual concurrency, male emigrants and men having sex with men form significant bridge populations who are appropriate subjects for targeted intervention. There is a critical need for increasing awareness about the benefits of circumcision and correct condom use as well as more intensive efforts at contact tracing.
| 1. |
Dudala SR. Updated Kuppuswamy′s socioeconomic scale for 2012. J NTR Univ Health Sci 2013;2:201-2.
[Google Scholar]
|
| 2. |
Al-Mutairi N, Joshi A, Nour-Eldin O, Sharma AK, El-Adawy I, Rijhwani M. Clinical patterns of sexually transmitted diseases, associated sociodemographic characteristics, and sexual practices in the Farwaniya region of Kuwait. Int J Dermatol 2007;46:594-9.
[Google Scholar]
|
| 3. |
Jain VK, Dayal S, Aggarwal K, Jain S. Changing trends of sexually transmitted diseases at Rohtak. Indian J Sex Transm Dis 2008;29:23-5.
[Google Scholar]
|
| 4. |
Maan MA, Hussain F, Iqbal J, Akhtar SJ. Sexually transmitted infections in Pakistan. Ann Saudi Med 2011;31:263-9.
[Google Scholar]
|
| 5. |
Wang B, Li X, Stanton B, Fang X, Lin D, Mao R. HIV-related risk behaviours and history of sexually transmitted diseases among male migrants who patronize commercial sex in China. Sex Transm Dis 2007;34:1-8.
[Google Scholar]
|
Fulltext Views
3,850
PDF downloads
1,764





![[Table - 1]](#tbl_ijdvl_2015_81_5_500_158646_t1.jpg){kind=link}
![[Figure - 1]](#fig_ijdvl_2015_81_5_500_158646_f2.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2015_81_5_500_158646_f3.jpg){kind=link}
![[Table - 2]](#tbl_ijdvl_2015_81_5_500_158646_t4.jpg){kind=link}
![[Table - 3]](#tbl_ijdvl_2015_81_5_500_158646_t5.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2015_81_5_500_158646_f6.jpg){kind=link}