Translate this page into:
Clinico-mycological study of dermatophytes in a tertiary care centre in northwest India
2 Mahatma Gandhi Medical College, Jaipur, Rajasthan, India
Correspondence Address:
U S Agarwal
397, Shankar Niwas, Shree Gopal Nagar, Gopalpura Bypass, Near Gurjar Ki Thadi, Jaipur, Rajasthan
India
| How to cite this article: Agarwal U S, Saran J, Agarwal P. Clinico-mycological study of dermatophytes in a tertiary care centre in northwest India. Indian J Dermatol Venereol Leprol 2014;80:194 |
Sir,
Superficial mycoses are infections of skin, hairs and nails caused by dermatophytes, yeasts and non-dermatophyte molds. Among these, dermatophytes are responsible for the largest number of cases. Dermatophytes are divided into three genera: Trichophyton, Epidermophyton and Microsporum. Distribution of the dermatophytes varies with the geographical area and course of time. [1]
We carried out this study to know the various epidemiological aspects of dermatophytoses in S.M.S. Hospital, Jaipur, a tertiary care center in northwest India.
A total of 300 clinically diagnosed patients of dermatophytoses attending the out-patient department during a 12 months period from November 2011 to October 2012 were registered. Patients who had taken antifungal treatment in the previous 1 month and those who did not provide informed consent were excluded. A detailed history coupled with a thorough clinical examination was carried out for each selected patient. Baseline investigations were performed to rule out any predisposing conditions. All specimens of skin, nail or hair scrapings and/or clippings were divided into 2 halves. One half was examined using 10% potassium hydroxide (KOH) solution while the other half was inoculated on Sabouraud′s dextrose agar with 0.05% chloramphenicol and Sabouraud′s dextrose agar with 0.05% chloramphenicol and 0.5% cycloheximide at 25°C for up to 4 weeks.
Patients were divided into six age groups; <10, 11-20, 21-30, 31-40, 41-50 and >50 year of age. The largest number of patients in our study, 91 (30.3%), were in the 21-30 year age group. Similar results were seen by other authors. [2],[3] Males (68.3%) outnumbered females (31.6%) with a male to female ratio of 2.16:1, which is similar to other studies. [3],[4] Patients were distributed into three disease duration groups, i.e.: <1 month, 1-3 months, >3 months. Most patients 163 (62.5%), had disease for longer than 3 months. The largest number of patients, 139 (46.33%) belonged to the lower middle class. Sarma and Borthakur [2] also found that most (60%) of their patients belonged to the lower middle class. In our study, the commonest occupation group affected was students (112, 37.3%) On the other hand, Sarma and Borthakur [2] found the disease most commonly in occupations related to agriculture (39%), followed by students and unskilled laborers (15%). Twenty eight (9.3%) patients had similar episodes in the past and 87 (27.7%) patients had been treated with medications other than antifungal drugs in the past.
Tinea corporis was the most common clinical pattern in 37.3% cases [Figure - 1], followed by mixed clinical pattern in 44 (14.7%), tinea cruris in 13.7% cases, tinea capitis in 39 (13%), onychomycosis in 33 (11%), tinea pedis in 11 (3.7%), tinea faciei in 9 (3%), tinea manuum in 6 (2%) and tinea barbae in 5 (1.7%) cases. As in other studies, [2],[3],[4] tinea corporis was the most common clinical pattern in our patients. Out of a total of 300 cases, 254 (84.67%) showed dermatophytes on KOH preparation and in 240 (80%) cases the fungus was grown on culture. Sahai and Mishra [3] reported similar dermatophyte demonstration and isolation rates of 89.6% and 83% respectively. The difference in these rates among different studies may be due to factors involved in the collection, transport and inoculation of specimens, culture conditions, severity, type and stage of disease and the effect of antifungal agents. Trichophyton mentagrophytes, grown in 91 (37.9%) cases was the most common isolate in our study [Figure - 2] and [Figure - 3] as also noted by Sahai and Mishra [3] On the other hand, a study conducted in 2008 in our geographical area by Jain et al. [5] found that Trichophyton rubrum was the most common dermatophyte. In our study, T. rubrum was grown in 82 (34.2%), Trichophyton violaceum in 27 (11.3%), Trichophyton tonsurans in 20 (8.3%), Microsporum audouinii in 15 (6.2%), Microsporum canis in 4 (1.7%), and Trichophyton verrucosum in 1 (0.4%) case. T. mentagrophytes was most common isolate in tinea corporis, tinea capitis and onychomycosis while T. rubrum was most common in tinea corporis with cruris.
 |
| Figure 1: Lesions of tinea corporis on back |
 |
| Figure 2: Colony of Trichophyton mentagrophytes |
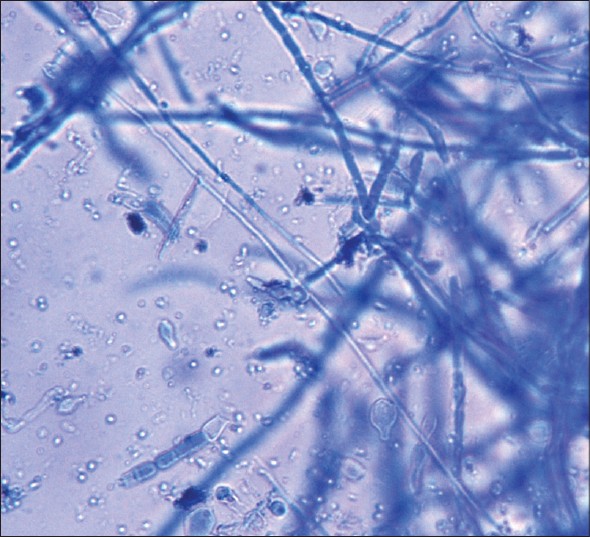 |
| Figure 3: Microscopic view of Trichophyton mentagrophytes |
The epidemiology of dermatophyte infections may change with time and studies such as this one provide information on the current status of the disease in a particular geographic area.
| 1. |
Seebacher C, Bouchara JP, Mignon B. Updates on the epidemiology of dermatophyte infections. Mycopathologia 2008;166:335-52.
[Google Scholar]
|
| 2. |
Sarma S, Borthakur AK. A clinico-epidemiological study of dermatophytoses in Northeast India. Indian J Dermatol Venereol Leprol 2007;73:427-8.
[Google Scholar]
|
| 3. |
Sahai S, Mishra D. Change in spectrum of dermatophytes isolated from superficial mycoses cases: First report from Central India. Indian J Dermatol Venereol Leprol 2011;77:335-6.
[Google Scholar]
|
| 4. |
Bindu V, Pavithran K. Clinico-mycological study of dermatophytosis in Calicut. Indian J Dermatol Venereol Leprol 2002;68:259-61.
[Google Scholar]
|
| 5. |
Jain N, Sharma M, Saxena VN. Clinico-mycological profile of dermatophytosis in Jaipur, Rajasthan. Indian J Dermatol Venereol Leprol 2008;74:274-5.
[Google Scholar]
|
Fulltext Views
3,169
PDF downloads
3,823





![[Figure - 1]](#fig_ijdvl_2014_80_2_194_129434_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2014_80_2_194_129434_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2014_80_2_194_129434_f3.jpg){kind=link}