Translate this page into:
Combination of A-T advancement flap and crescentic flap: A novel approach to repair surgical defect above the eyebrow
Correspondence Address:
Chih-Jung Hsu
Department of Dermatology, China Medical University Hospital, Taichung
Taiwan
| How to cite this article: Desale S, Hsu CJ. Combination of A-T advancement flap and crescentic flap: A novel approach to repair surgical defect above the eyebrow. Indian J Dermatol Venereol Leprol 2017;83:717-719 |
Sir,
An 86-year-old female patient was diagnosed with nodulocystic basal cell carcinoma (BCC), sized 1.3 × 1.0 cm, located above the left eyebrow after histopathology. The tumor was subjected to total excision with a narrow safety margin of 0.3 cm, under local anesthesia. Frozen section examination was performed intraoperatively to confirm free tumor margin. We designed a combination flap of A-T flap and crescentic flap [Figure 1a] for repairing the residual skin defect.
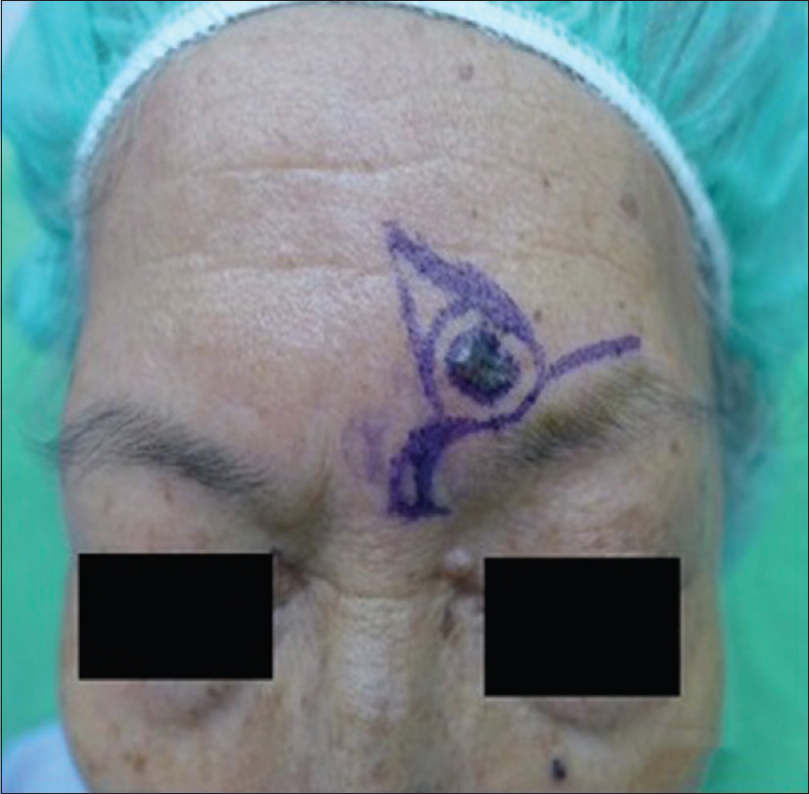 |
| Figure 1a: Preoperative image with markings for excision and method of repair |
After complete tumor resection, the residual oval skin defect was converted to triangular form with its base aligned along the superior border of the left eyebrow [triangle abc in [Figure 1b]. The incision was then extended bilaterally from the base of triangular defect to relieve the tension [bd and cg in [Figure 1b]. For compensation of unequal lengths we made burrow triangle on medial side of the eyebrow, which transformed into crescentic shape [Lunar shape skin “A” in [Figure 1b] to conceal the scar over the medial margin of eyebrow.
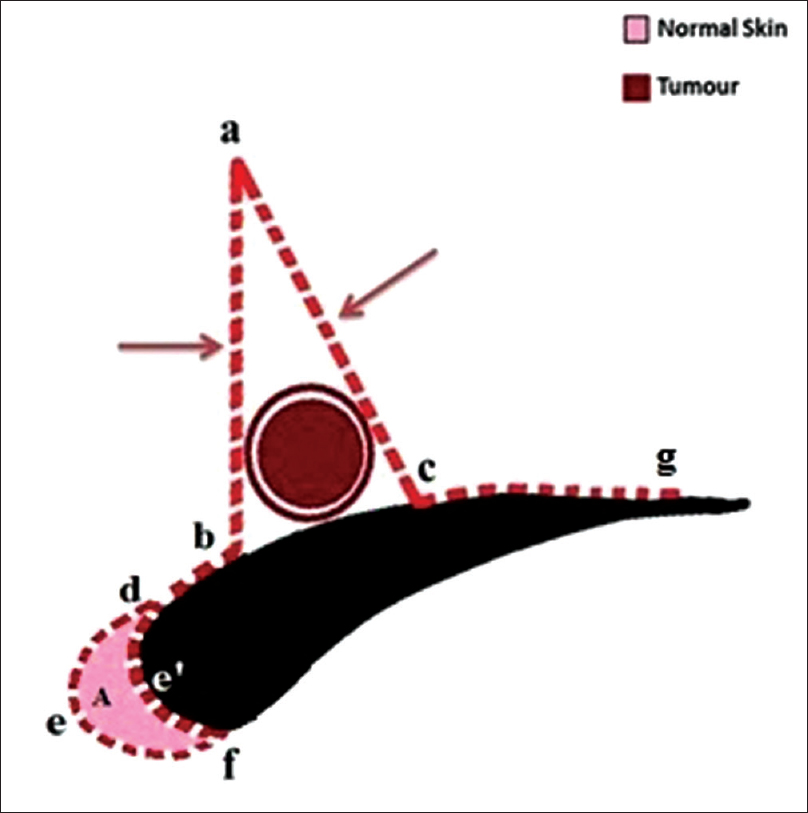 |
| Figure 1b: Illustration of combination of A-T and crescentic flap design. Triangle abc was created for reconstruction. Tension releasing incisions bd and cg were taken on each side of triangle. Crescent shape “A” with outer edge def and inner edge de'f was designed on medial margin of left eyebrow |
After undermining, two opposite flaps were approximated to centre on the base of the triangular defect and sutured in an inverted “T” shaped fashion [Figure 2a]. The vertical scar of the inverted “T” shape was easily obscured within the left glabellar crease [Figure 2b]. Base of the inverted T-shape closure was placed over the superior margin of the left eyebrow. The burrow triangle scar was placed on the medial border of eyebrow after lunar shape skin was removed. In this technique, two flaps were applied: A-T advancement flap over supra-eyebrow region and a crescentic flap over medial region, to maintain the symmetry of the eyebrows and to prevent folding of the left eyebrow. There were no postoperative complications except for ecchymosis over the nasal ridge and bilateral periorbital areas. These ecchymotic patches gradually faded over the next 2 weeks along with gradual healing of the reconstructed area.
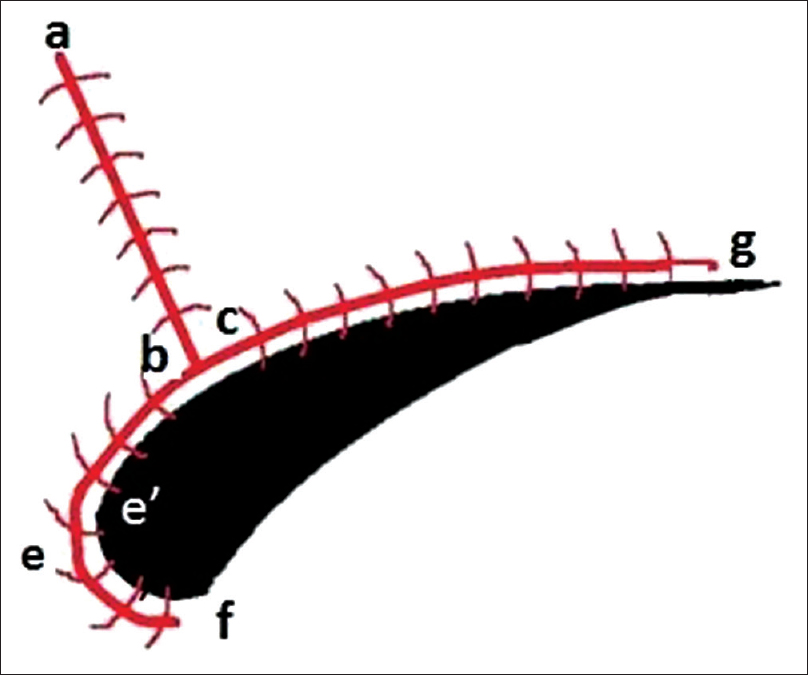 |
| Figure 2a: Illustration of combination of A-T and crescentic flap repair. The flaps “abd” and “acg” were approximated to centre on the base of the triangular defect and sutured to form an inverted “T” shape. The “bef” crescentic flap was then sutured to “ce'f” to complete the closure. The lateral extension of the incision “cg” was sutured |
 |
| Figure 2b: Immediate postoperative image with reconstruction using combination of A-T and crescentic flap |
After 12 months of follow-up, there was no evidence of local recurrence of BCC. Aesthetic appearance of the patient was acceptable without any eybrow asymmetry. Overall good scar resolution and satisfactory reconstruction was observed without disturbance of local anatomic structures (eyebrow and medial canthus) [Figure 2c].
 |
| Figure 2c: Repair with combination of A-T flap and crescentic flap 12 months after surgery |
The local flaps are more feasible options while treating facial defects; depending on skin tissue status (skin tension line, skin laxity, etc.), size and location of the skin defect.[1] Rotational flaps, transposition flaps, and advancement flaps are three basic types of local flaps.
The advancement flap is one of the most basic and versatile flaps used by dermatosurgeons.[2],[3] The advancement flap simply involves the linear advancement of tissue in one direction. Advancement flaps involve wide range of flap designs such as H flap, A-T flap, and crescentic flap.
A-T flap involves conversion of original circular defect into triangular defect and placing two tension releasing incisions tangentially on the superior or inferior aspect of circular defect. Burrow triangle may be created either on one side of the defect or both sides depending on size of skin defect or its elasticity. In this flap method, incisions are made perpendicular to a linear repair axis to avoid crossing the cosmetic unit boundary. Individual A-T advancement flap, crescentic flap, and/or their modifications are commonly used to treat facial defects in dermato-surgery.[4] However, a combination of two flap techniques has not been reported previously, to the best of our knowledge. The defects on supra-eyebrow area are difficult to reconstruct as the slightest error in judgment leads to eyebrow interruption and noticeable eyebrow asymmetry and or deformity. Hence, to achieve better cosmesis, we reconstructed the defect with the combination of crescentic flap and A-T flap. Crescent shaped design made the burrow triangle following the anatomic curve of eyebrow. Scar line was concealed in the medial side of eyebrow. Traditional A-T flap design not only avoids interruption of eyebrow but also hides the “inverse T” scar inside the inherent glabellar wrinkle and the superior margin of eyebrow. The perfect composition of two flaps achieved benefit of invisible postoperative scar with well-accepted cosmetic appearance.
In conclusion, eyebrow defects following local tumor excision require a suitable technique to restore symmetry and cosmesis. Combination of A-T flap and crescentic flap is a safe and feasible alternative to close larger eyebrow defects without interruption of eyebrow. With this combination flap, one can eliminate the risk of eyebrow deformity such as the folding or bulging. Advantages of this combination flap technique are the ability to hide the scar in glabellar wrinkle line and border of eyebrow while maintaining eyebrow symmetry.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient has given her consent for her images and other clinical information to be reported in the journal. The patient understands that name and initial will not be published and due efforts will be made to conceal identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Beasley NJ, Gilbert RW, Gullane PJ, Brown DH, Irish JC, Neligan PC, et al. Scalp and forehead reconstruction using free revascularized tissue transfer. Arch Facial Plast Surg 2004;6:16-20.
[Google Scholar]
|
| 2. |
Krishnan R, Garman M, Nunez-Gussman J, Orengo I. Advancement flaps: A basic theme with many variations. Dermatol Surg 2005;31:986-94.
[Google Scholar]
|
| 3. |
Harris GJ, Garcia GH. Advancement flaps for large defects of the eyebrow, glabella, forehead, and temple. Ophthal Plast Reconstr Surg 2002;18:138-45.
[Google Scholar]
|
| 4. |
Birgfeld CB, Chang B. The periglabellar flap for closure of central forehead defects. Plast Reconstr Surg 2007;120:130-3.
[Google Scholar]
|
Fulltext Views
4,037
PDF downloads
2,496




