
Translate this page into:
Comparative analysis of the facial microbiome between rosacea and seborrheic dermatitis
Corresponding author: Dr. Ruojun Wang, Department of Dermatology, Peking University First Hospital, Beijing, China wangrj@bjmu.edu.cn
-
Received: ,
Accepted: ,
How to cite this article: Tao R, Li R, Wang R. Comparative analysis of the facial microbiome between rosacea and seborrheic dermatitis. Indian J Dermatol Venereol Leprol 2023;89:891-3.
Dear Editor,
Rosacea and seborrheic dermatitis are both common chronic inflammatory dermatoses of the face or scalp. These two conditions share some common features in clinical manifestations. Patients with seborrheic dermatitis usually present with erythematous patches with greasy scales, whereas rosacea is characterized by persistent facial erythema, telangiectasia, papules and pustules in different stages.1,2 Since the two diseases might be hard to differentiate in some cases, clinical studies have focused on other distinct pathogenetic characteristics to help with their diagnosis and treatment. Current studies have shown that micro-ecological disequilibrium plays a role in the development of both.1,2 In this study, we aim to characterise and compare the bacterial and fungal microbiomes in skin of patients with rosacea and seborrheic dermatitis.
The amplicon sequencing data of 18 rosacea patients, 18 patients with facial seborrheic dermatitis and 11 healthy individuals who visited the Department of Dermatology at Peking University First Hospital, Beijing, China, from 1st January 2018 to 31st August 2021 were obtained from the previous datasets.3,4 This study was approved by the Institutional Review Boards of Peking University First Hospital, Beijing, China, and informed written consent was obtained from all the participants. All skin samples were collected from the cheeks. Deoxyribonucleic acid (DNA) extraction and sequencing of the bacterial 16S ribosomal ribonucleic acid (rRNA) and fungal internal transcribed spacer 1–5F regions were performed as described in the supplementary material. Disease severity of seborrheic dermatitis and rosacea were assessed based on clinical presentations and transepidermal water loss levels were examined using a Vapometer (Delfin Technologies, Italy). Categorical data were compared by the chi-squared test and community differences were analysed using the Wilcoxon test for two-group comparisons and the Kruskal–Wallis test for multigroup comparisons. The results of all the analyses were displayed in ‘R software’ (version 3.6.1). There were no significant differences with respect to age and gender between the groups (Table 1).
| SD | Rosacea | HC | |
|---|---|---|---|
| Number | 18 | 18 | 11 |
| Age | 34.8 ± 17.5 | 35.7 ± 9.0 | 36.0 ± 13.6 |
| Gender (Female:male) | 5:4 | 7:2 | 5:6 |
| Disease diversity (percentage of moderate/severe) | 72.2% | 50.0% | N/A |
| Transepidermal water loss | 73.2 ± 43.9 | 23.3 ± 8.8 | 19.5 ± 10.6 |
SD: seborrheic dermatitis, HC: healthy control, TEWL: transepidermal water loss
The Shannon diversity index, which reflects the richness and evenness of a microbial community, was calculated.3 The bacterial and fungal Shannon diversities were significantly decreased in the seborrheic dermatitis group compared to the rosacea group and controls and the bacterial Shannon diversity was increased in the rosacea group compared to the controls [Figure 1]. Bacterial taxonomic analyses revealed that Actinobacteria and Firmicutes were the dominant bacterial phyla in all groups. The abundance of Firmicutes was increased, and the abundance of Actinobacteria was decreased in seborrheic dermatitis and rosacea groups compared to the controls. At the genus level, the relative abundance of Cutibacterium was significantly decreased in seborrheic dermatitis (37.8%) and rosacea (21.7%) groups compared to the controls (63.5%, Kruskal–Wallis test, P < 0.01), while the relative abundance of Staphylococcus was significantly higher in the seborrheic dermatitis group (35.9%) than in the controls (8.4%, P < 0.001). Comparative analysis revealed an increased relative abundance of Cutibacterium (P < 0.05) and a decreased relative abundance of Streptococcus (seborrheic dermatitis group vs rosacea group: 0.6 vs 23.3%, P < 0.05) in the seborrheic dermatitis group compared with the rosacea group [Figure 2].
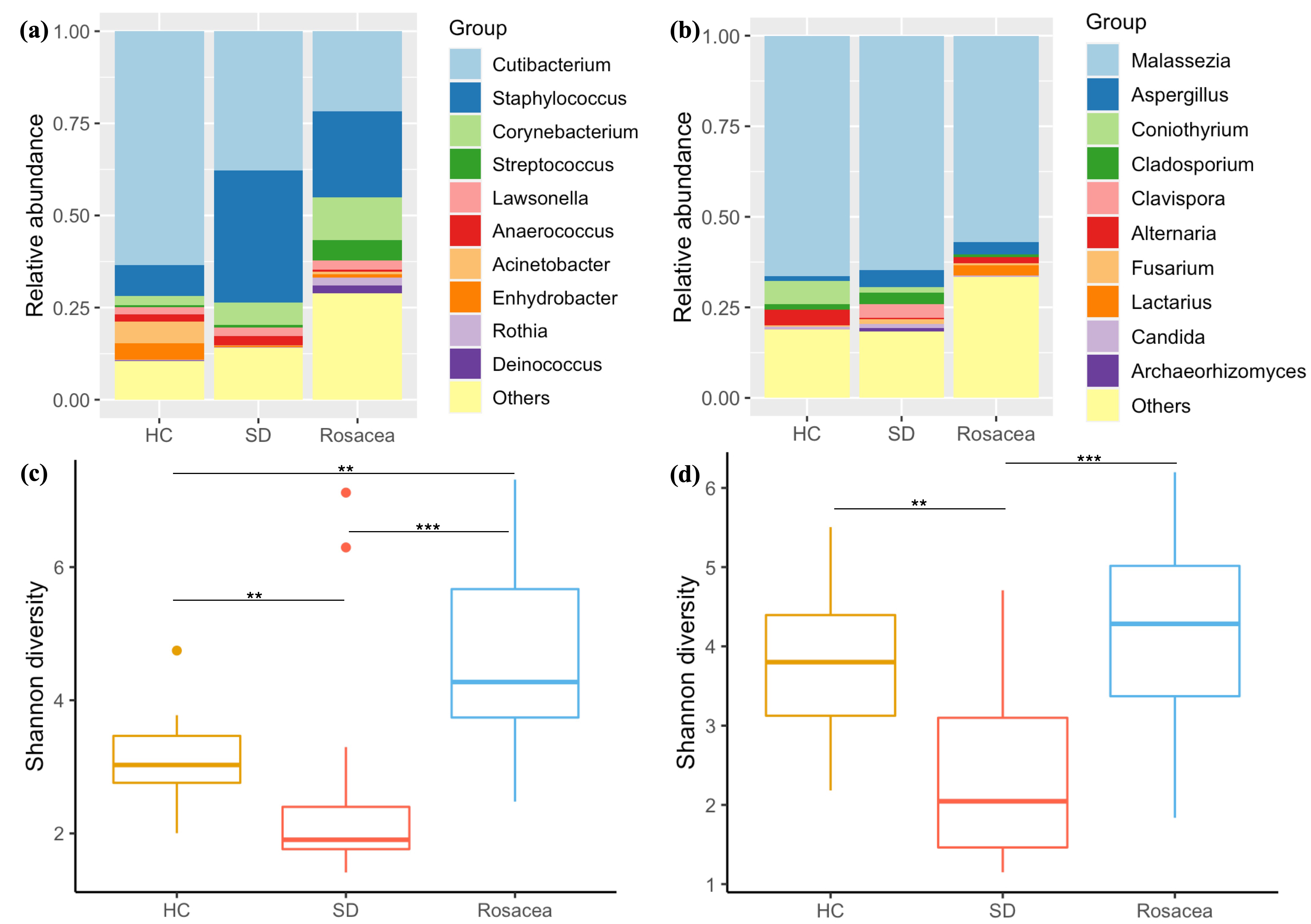
- Relative abundances of bacterial (a) and fungal taxa (b) at the genus level in different groups. Only the top 10 enriched genera taxa are shown. Shannon diversity of the bacterial (c) and fungal (d) communities in the seborrheic dermatitis group, rosacea group and controls. SD: seborrheic dermatitis, HC: healthy control *P < 0.05; **P < 0.01; ***P < 0.001
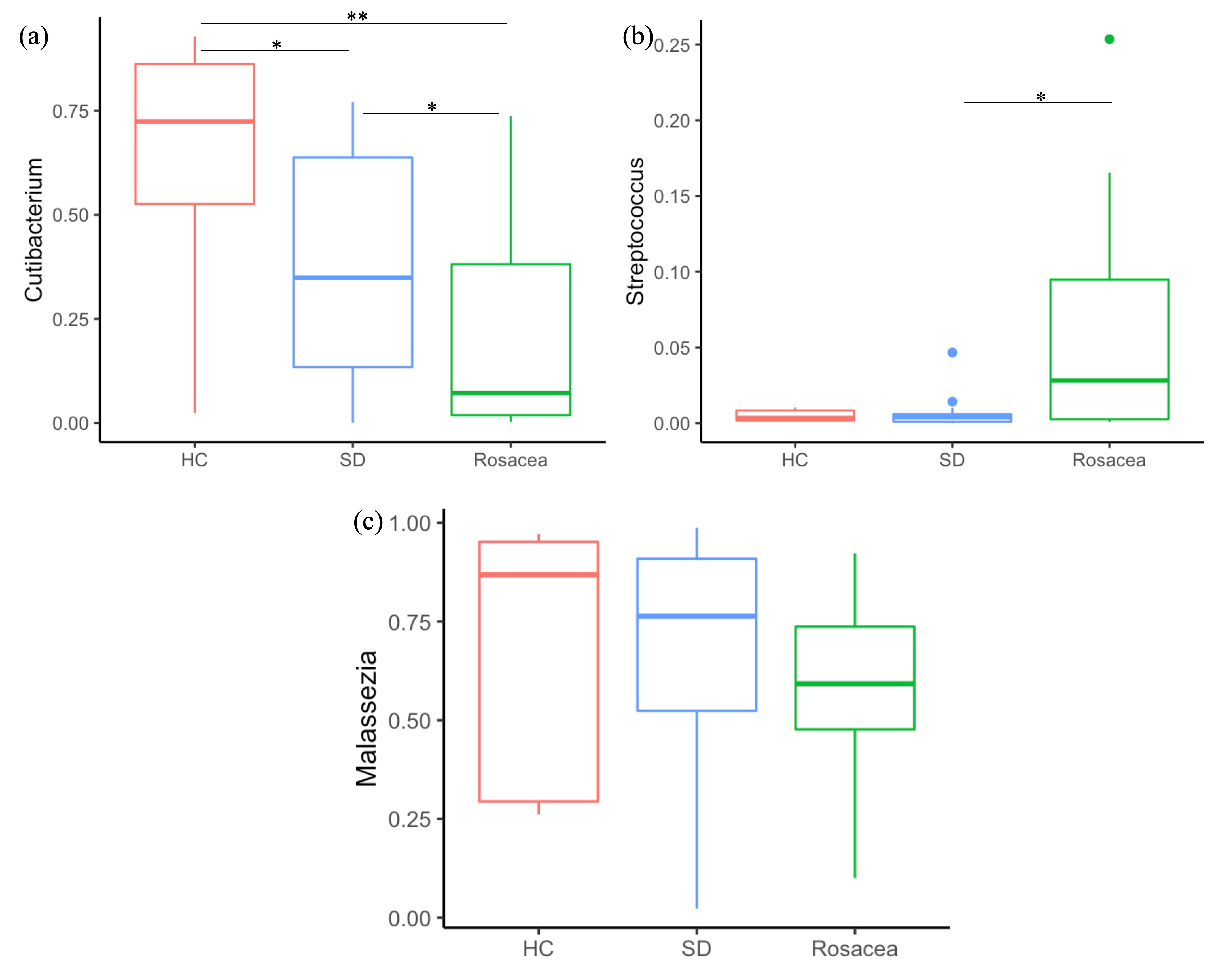
- Relative abundances of Cutibacterium, Streptococcus and Malassezia in the seborrheic dermatitis group, rosacea group and controls. SD: seborrheic dermatitis, HC: healthy control *P < 0.05, **P < 0.01, ***P < 0.001
On examination of the fungal taxa, the dominant phyla were Basidiomycota and Ascomycota. At the genus level, although we found an increasing trend in the abundance of Malassezia in the seborrheic dermatitis group (64.8%) compared with the rosacea group (56.9%), no statistical significance could be detected. We also observed an increase in the relative abundance of Coniothyrium (seborrheic dermatitis group vs rosacea group: 1.5 vs 0.0%, P < 0.001) and a decrease in the relative abundance of Alternaria (seborrheic dermatitis group vs rosacea group: 0.3 vs 1.7%, P < 0.01) in the seborrheic dermatitis group compared to the rosacea group. At the species level, an increasing trend in the abundance of Malassezia globosa was found in the seborrheic dermatitis group compared with the rosacea group (no statistical significance). We also found a significant reduction in the abundance of Alternaria alternata and an increase in the abundance of Aspergillus microcysticus in the seborrheic dermatitis group, compared to the controls. However, the rosacea group did not show significant differences in the predominant fungal taxa in comparison to controls.
In the analysis of the correlation between clinical parameters and microbial taxa, the disease severity of seborrheic dermatitis was found to be positively correlated with Malassezia and Aspergillus and negatively correlated with Staphylococcus, whereas the disease severity of rosacea was positively correlated with Streptococcus and negatively correlated with Malassezia. No significant correlation was found between degree of transepidermal water loss and microbial taxa.
The proportion of certain pathogenic and protective microorganisms has been found to be altered in the facial skin microbiome in patients with rosacea and seborrheic dermatitis.1,2 Our results suggest that these two conditions involve different patterns of skin microbial dysbiosis. Seborrheic dermatitis is associated with imbalanced fungal and bacterial communities, whereas rosacea is more likely to be related to dysbiosis of solely the bacterial community. Therapies targeting potential pathogenic microbes could probably aid in the treatment of both conditions. This study is mainly limited by the relatively small number of participants. Efforts were made to minimise potential bias: age and sex were matched between groups and the sampling methods and skin sites were consistent. Future interventional studies with greater sample sizes will be useful to explain the role of microbes in the pathophysiology of seborrheic dermatitis and rosacea and whether therapies modulating the microbiome are effective for the treatment of the two diseases.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflict of interest
There are no conflicts of interest.
References
- Skin microbiome alterations in seborrheic dermatitis and dandruff: A systematic review. Exp Dermatol. 2021;30:1546-53.
- [CrossRef] [PubMed] [Google Scholar]
- Rosacea and the microbiome: A systematic review. Dermatol Ther (Heidelb). 2021;11:1-12.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Bacterial and fungal microbiome characterisation in patients with rosacea and healthy controls. Br J Dermatol. 2020;183:1112-4.
- [CrossRef] [PubMed] [Google Scholar]
- Ketoconazole 2% cream alters the skin fungal microbiome in seborrheic dermatitis: A cohort study. Clin Exp Dermatol. 2022;47:1088-96.
- [CrossRef] [PubMed] [Google Scholar]




