Translate this page into:
Concurrent lichen scrofulosorum and papulonecrotic tuberculid in a patient with tubercular lymphadenitis
Correspondence Address:
Pravesh Yadav
RZ 97, Phase III, Prem Nagar, Najafgarh, New Delhi - 110 043
India
| How to cite this article: Yadav P, Mendiratta V, N, Chander R. Concurrent lichen scrofulosorum and papulonecrotic tuberculid in a patient with tubercular lymphadenitis. Indian J Dermatol Venereol Leprol 2014;80:483 |
Sir,
A 14-year-old girl was seen for crops of intensely itchy, skin-colored papules, some of which healed with scars, over the trunk and limbs since two and a half months. She complained of rise in temperature in the evening, weight loss and loss of appetite. She had had pulmonary tuberculosis at the age of six years for which she had received complete treatment. Her mother had tubercular lymphadenitis ten years back which was adequately treated.
Cutaneous examination revealed multiple, grouped, tiny, skin-colored follicular and extrafollicular papules with minimal scaling over the back, abdomen and proximal extremities [Figure - 1]. Multiple discrete, slightly erythematous to hyperpigmented 4 to 5 mm papules with necrotic centers were noticed over the dorsum and medial aspect of the feet, extensor aspect of legs and extensor aspect of both forearms [Figure - 2]. Multiple, matted lymph nodes in the right anterior cervical group were present [Figure - 3]. Systemic examination was normal.
 |
| Figure 1: Multiple grouped pinhead size skin colored follicular as well as extrafollicular papules with minimal scaling involving the back |
 |
| Figure 2: Multiple discrete, slightly erythematous to hyperpigmented papules with necrotic center over the medial aspect of the feet |
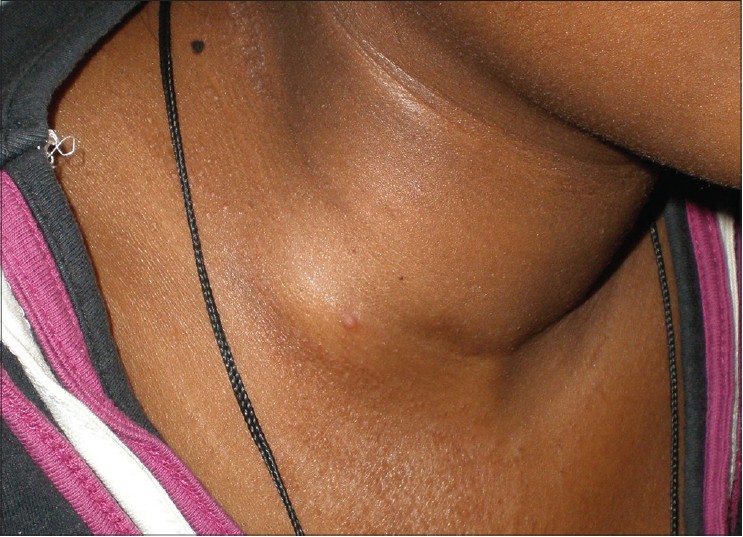 |
| Figure 3: Matted lymph nodes in the right anterior cervical group |
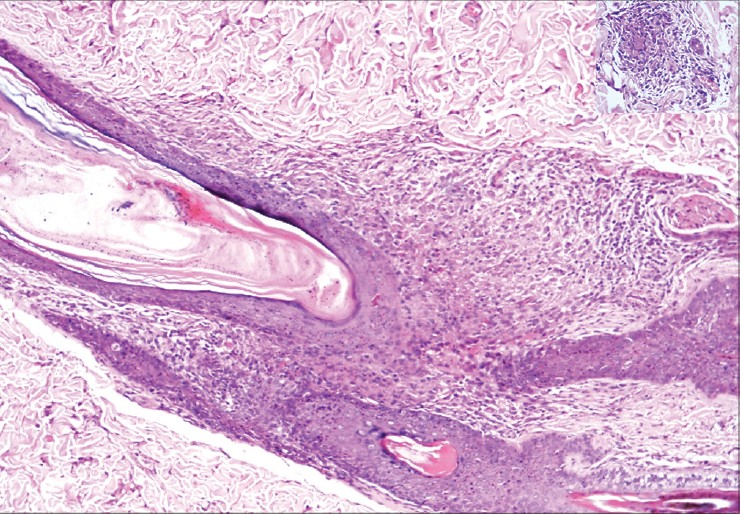
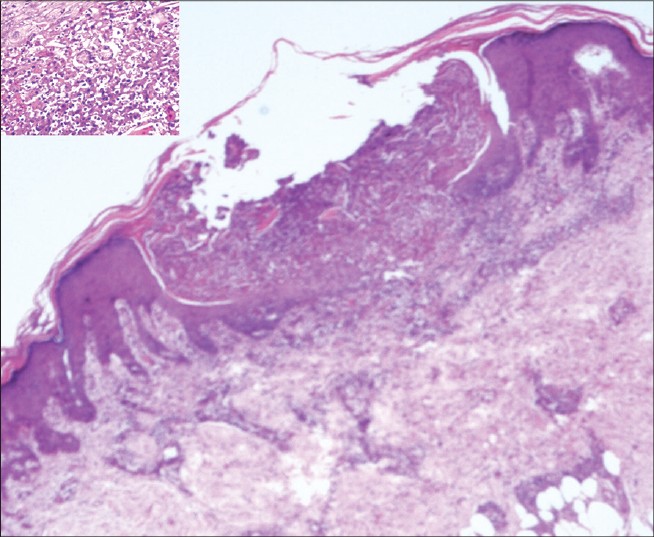
The Mantoux test was strongly positive with an induration of 30 mm at 48 hours. Hematological and routine biochemical tests were normal except for a raised erythrocyte sedimentation rate (ESR) of 108 mm. Skin biopsy from the trunk lesions showed non-caseating epithelioid cell granulomas predominantly in the perifollicular and periadnexal region, suggestive of lichen scrofulosorum [Figure - 4] . Biopsy from a larger, centrally necrotic papule on the leg revealed a wedge shaped area of necrosis with its broad base towards epidermis. Epitheloid cells and Langhans giant cells were seen around the periphery of the necrosis along with features of leukocytoclastic vasculitis suggestive of papulonecrotic tuberculid [Figure - 5] . Modified Ziehl-Neelsen stain did not show acid fast bacilli in both biopsies. Fine needle aspiration cytology from the right anterior cervical lymph node showed features suggestive of tubercular lymphadenitis and acid fast bacilli were noted. Radiograph of the chest showed widening of the mediastinum suggestive of mediastinal lymphadenopathy. Ultrasound of the abdomen revealed a few enlarged, matted retroperitoneal lymph nodes up to 2.5 cm in size.
 |
| Figure 4: Non-caseating epithelioid cell granulomas with Langhans giant cells in the perifollicular region. (H and E, ×10) INSET: Closer view (H and E, ×40) |
 |
| Figure 5: Wedge shaped area of necrosis with its broad base towards epidermis. Epithelioid cells and langhans giant cells around the periphery of necrosis along with features of leukocytoclastic vasculitis. (H and E, ×4) INSET: Closer view (H and E, ×40) |
The patient was started on World Health Organization recommended directly observed therapy short course (DOTS) Category II antitubercular treatment (ATT) with 5 drugs (oral isoniazid, rifampin, ethambutol, pyrazinamide and injectable streptomycin). There was a rapid response with improvement in itching within two weeks of starting therapy. The itch had not responded previously to oral antihistamines. Skin lesions improved over the next two months whereas the lymph nodes resolved in six months.
Tuberculids are thought to be due to hematogenous spread of bacilli in a person with a moderate or high degree of immunity against Mycobacterium tuberculosis. The factors that determine the type of presentation are still to be elucidated. One of the possible factors is the fluctuation in the immunological state of the patients. Mycobacterial DNA had not been detected from lichen scrofulosorum lesions till recently, [1] while it has been demonstrated by polymerase chain reaction in skin lesions of papulonecrotic tuberculid and nodular forms. This finding had led to the suggestion that papular and nodular forms of tuberculid should be regarded as forms of true post-primary tuberculosis. [2]
The coexistence of lichen scrofulosorum and papulonecrotic tuberculid has been described earlier in three case reports. Wechsler in 1951 reported concomitant papulonecrotic tuberculid and lichen scrofulosorum in a patient. [3] Thappa et al., [4] reported a child with transformation from papulonecrotic tuberculid to lichen scrofulosorum, however the lesions of papulonecrotic tuberculid had already resolved at the time of presentation to the physician and the diagnosis was made on the basis of healed scars. A 29-year-old male with both papulonecrotic tuberculid and lichen scrofulosorum without any known focus of tuberculosis was reported recently. [5]
An interesting aspect of our case was the severe itch which did not respond to antihistamines but was relieved with anti-tubercular therapy.
| 1. |
Ben Jazia E, Hachfi W, Trimech M, Hmissa S, Jeddi CH, Omezzine-Letaief A. Detection of mycobacterial tuberculosis DNA in lichen scrofulosorum. J Am Acad Dermatol 2006;55:S54-5.
[Google Scholar]
|
| 2. |
Degitz K, Steidl M, Thomas P, Plewig G, Volkenandt M. Aetiology of tuberculids. Lancet 1993;341:239-40.
[Google Scholar]
|
| 3. |
Wechsler HL. Tuberculosis of axillary lymph nodes; phlyctenular keratitis; lichen scrofulosorum; papulonecrotic tuberculide; erythema induratum. AMA Arch Derm Syphilol 1951;64:508-9.
[Google Scholar]
|
| 4. |
Thappa DM, Karthikeyan K, Jayanthi S. Tuberculid in a child: Transformation from papulonecrotic to lichen scrofulosorum. Pediatr Dermatol 2003;20:91-3.
[Google Scholar]
|
| 5. |
Das JK, Sengupta S, Mitra S, Gangopadhyay AK. Coexistence of papulonecrotic tuberculide with lichen scrofulosorum. Indian J Dermatol 2010;55:109-12.
[Google Scholar]
|
Fulltext Views
3,328
PDF downloads
1,841





![[Figure - 1]](#fig_ijdvl_2014_80_5_483_140347_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2014_80_5_483_140347_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2014_80_5_483_140347_f3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2014_80_5_483_140347_f4.jpg){kind=link}
![[Figure - 5]](#fig_ijdvl_2014_80_5_483_140347_f5.jpg){kind=link}