Translate this page into:
Congenital alopecia of eyebrow
2 Department of Dermatology and STD, University College of Medical Sciences and GTB Hospital, Delhi, India
Correspondence Address:
Chander Grover
Department of Dermatology and STD, University College of Medical Sciences and GTB Hospital, Dilshad Garden, Delhi
India
| How to cite this article: Jakhar D, Grover C. Congenital alopecia of eyebrow. Indian J Dermatol Venereol Leprol 2018;84:743-744 |
Sir,
A 10-year-old boy presented with absence of hair in a linear pattern on the right eyebrow noticed since birth. The child was born out of a nonconsanguineous marriage at full term by spontaneous vaginal delivery. There was no history of any maternal drug intake during pregnancy or instrumentation during delivery. There was no history of trauma, scarring or any other similar family history.
On examination, a single well-demarcated, linear patch (3 cm × 0.5 cm) of noncicatricial alopecia was present on the right eyebrow [Figure - 1]. The overlying skin was normal without any atrophy, inflammation or desquamation. Surrounding hair was normal and hair pull test was negative. Dermoscopy revealed the presence of a few vellus hair surrounded by normal hair [Figure - 2]a and [Figure - 2]b. There were no yellow dots or black dots. Pigtail hair, broken hair or exclamation mark hair were not seen. No other mucocutaneous or systemic abnormalities were noted. It was diagnosed as congenital alopecia, however, parents did not consent for a skin biopsy. Patient was followed up for another 1 year during which no clinical or trichoscopic changes were observed.
 |
| Figure 1: A linear patch of alopecia in the right eyebrow of a 10-year-old boy |
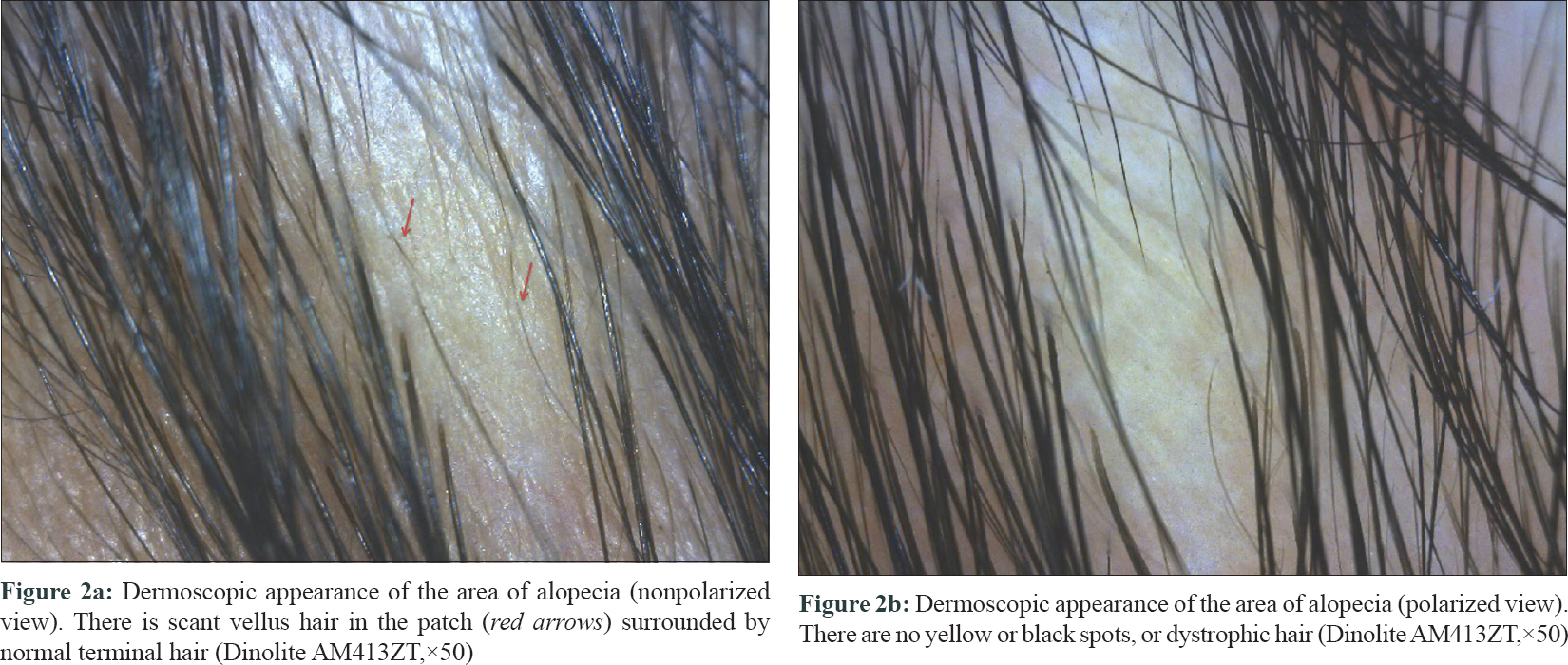 |
| Figure 2: |
Congenital alopecia, also known as Brauer nevus or temporal triangular alopecia, was first described in 1905 by Sabouraud.[1] Since then, there are numerous reports in the literature. The original term “congenital alopecia” or “temporal triangular alopecia” is now considered inadequate as the entity is neither congenital nor triangular in all the cases.[2] Though initially and classically described in the fronto-temporal region, it can also be seen on the temporo-parietal, occipital and vertex areas.[3] Congenital alopecia has been classically described as lacking any hair, although a few normal terminal or vellus hair may be evident within the affected patch.[4] Although, it is usually unilateral, bilateral involvement has also been described.[4] There is no gender predilection and the patch remains unchanged over the lifetime.[4]
Histopathology has been reported to show a normal number of follicles with a predominance of vellus hair, but occasional terminal hair in the superficial dermis, without any evidence of inflammation or scarring.[4],[5] Trichoscopy shows presence of vellus hair with normal follicular openings, and terminal hair at the unaffected normal area. Black and/or yellow dots and “exclamation mark” hair are absent.[5] Alopecia areata is a close differential diagnosis and absence of black dots, yellow dots, broken hair and exclamation mark hair on trichoscopy helps to differentiate this condition.[5]
Diagnostic criteria proposed for congenital alopecia include: (1) triangular or spear-shaped area of alopecia involving the fronto-temporal region of scalp; (2) normal follicular openings with vellus hair surrounded by normal terminal hair on dermoscopy; (3) absence of yellow and black spots, dystrophic hair or decreased follicular openings on dermoscopy; (4) no significant growth of hair even after dermoscopic and clinical confirmation of the existence of vellus hair.[2],[5] In most cases no therapeutic intervention is required and adequate counseling suffices. Therapeutic modalities include surgical excision, hair transplantation and topical minoxidil.[3],[4],[5]
Our case had typical diagnostic features of congenital alopecia, but at a unique location. An extensive search of literature did not reveal any similar reports. We believe that this may be an overlooked or under-reported entity. Our report may serve to make clinicians familiar with this entity and similar such reports may not be a surprise in future.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the parents have given their consent for images and other clinical information to be reported in the journal. The parents understand that name and initials will not be published and due efforts will be made to conceal patient identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Yin Li VC, Yesudian PD. Congenital triangular alopecia. Int J Trichology 2015;7:48-53.
[Google Scholar]
|
| 2. |
Campos JG, Oliveira CM, Romero SA, Klein AP, Akel PB, Pinto GM. Use of dermoscopy in the diagnosis of temporal triangular alopecia. An Bras Dermatol 2015;90:123-5.
[Google Scholar]
|
| 3. |
Singh N, Goyal A, Thappa DM, Rajesh NG. Congenital triangular alopecia: Is it always confined to fronto-temporal region? Indian J DermatolVenereolLeprol 2016;82:112.
[Google Scholar]
|
| 4. |
Yamazaki M, Irisawa R, Tsuboi R. Temporal triangular alopecia and a review of 52 past cases. J Dermatol 2010;37:360-2.
[Google Scholar]
|
| 5. |
Inui S, Nakajima T, Itami S. Temporal triangular alopecia: Trichoscopic diagnosis. J Dermatol 2012;39:572-4.
[Google Scholar]
|
Fulltext Views
6,056
PDF downloads
1,598





![[Figure - 1]](#fig_ijdvl_2018_84_6_743_242672_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2018_84_6_743_242672_f2.jpg){kind=link}