Translate this page into:
Congenital triangular alopecia: Is it always confined to fronto-temporal region?
2 Department of Pathology, Jawaharlal Institute of Postgraduate Medical Education and Research, Puducherry - 605 006, India
Correspondence Address:
Nidhi Singh
Assistant Professor, Department of Dermatology, Jawaharlal Institute of Postgraduate Medical Education and Research, Puducherry - 605 006
India
| How to cite this article: Singh N, Goyal A, Thappa DM, Rajesh NG. Congenital triangular alopecia: Is it always confined to fronto-temporal region?. Indian J Dermatol Venereol Leprol 2016;82:112 |
Sir,
Congenital triangular alopecia (CTA) is widely known as temporal triangular alopecia and presents as non-scarring, non-inflammatory triangular, oval or lancet shaped alopecia confined to the fronto-temporal scalp.[1] It is also known as Brauer nevus and was first described by Sabouraud in 1905.[2] We report congenital triangular alopecia over the left temporo-parieto-vertex region of scalp.
A 1-year-old girl, born of a second degree consanguineous marriage presented with triangular alopecia on the scalp since birth. She was delivered at term by spontaneous vaginal delivery. No instruments or fetal scalp electrodes had been used during delivery. There was no history of trauma or raw areas present over the scalp at birth. There was no family history of similar disorders. The child was subjected to repeated tonsuring over 1 year, with a hope of hair regrowth in the area of alopecia. Examination revealed a well-demarcated, 13 × 12 × 10 cm triangular patch of non-scarring alopecia occupying the left temporo-parieto-vertex region of scalp [Figure - 1]a, which on dermoscopy revealed normal follicular openings and vellus hair [Figure - 1]b. Hair pull test at the periphery of the patch was negative. No other abnormality of skin or nail was noted. Skin biopsy from the patch of alopecia revealed a few telogen vellus hair follicles, which were miniaturized. There was no perifollicular inflammation and scarring. [Figure - 2]a and [Figure - 2]b. The parents were informed regarding the option of hair transplantation as the patch was large and scarring was a possible sequel of staged excision of the patch.
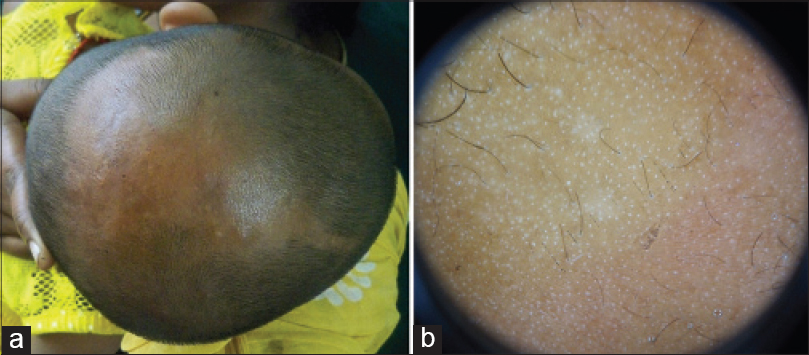 |
| Figure 1: (a) Triangular patch of nonscarring alopecia over left temporo-parieto-vertex region of scalp; (b) Dermoscopy showing normal follicular openings and vellus hairs |
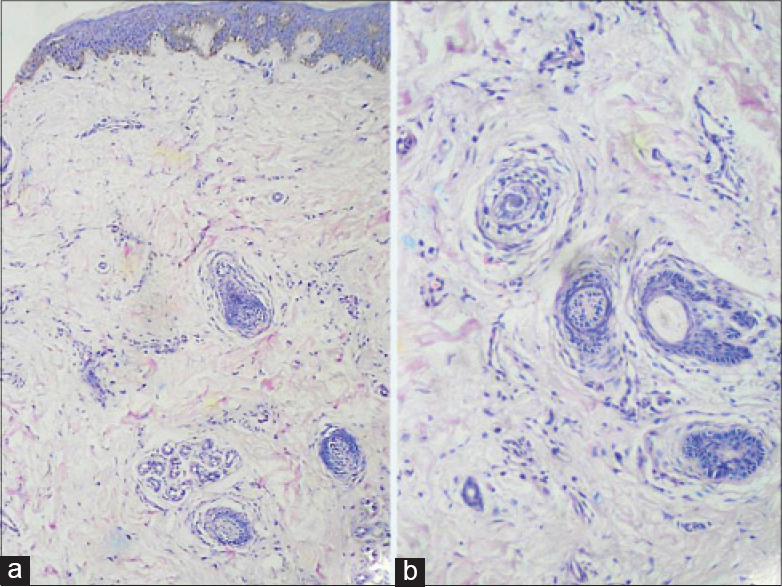 |
| Figure 2: Miniaturized telogen hair in dermis with no evidence of scarring or perifollicular inflammation in (a) low, and (b) higher magnification (Hematoxylin and Eosin stain, x40 and ×200, respectively) |
Congenital triangular alopecia has been consistently described in the fronto-temporal region of scalp. There are reports of variable shapes of alopecia, which need not necessarily be triangular. It is usually unilateral (80%) and has been more commonly described on the left side and rarely described bilaterally. More than half the cases have been noticed between 2 and 9 years of age, while a little more than one-third of the cases have been noticed at birth. It is characterized by the presence of vellus hairs.[1] It is a developmental defect that was once considered congenital but now many consider to be acquired.[3] It is usually sporadic but rarely may occur in families and is considered to be a paradominant trait.[4]
It may be misdiagnosed as alopecia areata, traction alopecia, trichotillomania, tinea capitis and aplasia cutis congenita. These can be easily differentiated using dermoscopy which would reveal normal follicular openings and vellus hairs in the patch of alopecia of congenital triangular alopecia.[5] On histopathology, absence of mature hair follicles and presence of vellus hairs give an appearance of “miniaturized hair follicles” as seen in androgenetic alopecia.[1] Complete excision may be considered for small lesions, while others would require hair restoration surgery.[3] Although some cases have been reported from India,[6] we report this case to highlight the rare occurence of large triangular patch of alopecia, involving the parietal, temporal and vertex regions of the scalp.
| 1. |
Yamazaki M, Irisawa R, Tsuboi R. Temporal triangular alopecia and a review of 52 past cases. J Dermatol 2010;37:360-2.
[Google Scholar]
|
| 2. |
García-Hernández MJ, Rodríguez-Pichardo A, Camacho F. Congenital triangular alopecia (Brauer nevus). Pediatr Dermatol 1995;12:301-3.
[Google Scholar]
|
| 3. |
Erickson Q, Yanase D, Perry V. Temporal triangular alopecia: Report of an African-American child with TTA misdiagnosed as refractory tinea capitis. Pediatr Dermatol 2002;19:129-31.
[Google Scholar]
|
| 4. |
Happle R. Congenital triangular alopecia may be categorized as a paradominant trait. Eur J Dermatol 2003;13:346-7.
[Google Scholar]
|
| 5. |
Iorizzo M, Pazzaglia M, Starace M, Militello G, Tosti A. Videodermoscopy: A useful tool for diagnosing congenital triangular alopecia. Pediatr Dermatol 2008;25:652-4.
[Google Scholar]
|
| 6. |
Kudligi C, Bhagwat PV, Eshwarrao MS, Tandon N. Giant congenital triangular alopecia mimicking alopecia areata. Int J Trichology 2012;4:51-2.
[Google Scholar]
|
Fulltext Views
3,940
PDF downloads
2,946





![[Figure - 1]](#fig_ijdvl_2016_82_1_112_157456_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2016_82_1_112_157456_f2.jpg){kind=link}