Translate this page into:
Cutaneous CD4+/ CD56 hematodermic neoplasm
2 Department of Pathology, Istanbul, Turkey
Correspondence Address:
Ilkin Zindanci
Goztepe Training and Resach Hospital, Department of Dermatology, Istanbul
Turkey
| How to cite this article: Zindanci I, Kavala M, Buyukbabani N, Kocaturk E, Koc M. Cutaneous CD4+/ CD56 hematodermic neoplasm. Indian J Dermatol Venereol Leprol 2010;76:723 |
Abstract
CD4+/CD56+ hematodermic neoplasm, formerly known as blastic NK cell lymphoma, is a rare and aggressive neoplasm with a high incidence of cutaneous involvement, risk of leukemic dissemination and poor prognosis. The characteristic features are expression of the T helper inducer cell marker CD4 and the NK-cell marker CD56 in the absence of other T cell or NKcell specific markers. Because of the rarity of this disease, we describe a 48 year old woman suffering from CD4+/CD56+ hematodermic neoplasm on her cheek without leukemic infiltration.Introduction
CD4+/CD56+ hematodermic neoplasm (HN), also termed as blastic natural killer (NK) cell lymphoma, is an aggressive systemic neoplasm commonly involving the skin. [1] It usually presents as either solitary or multiple nodules; systemic involvement of lymph nodes or bone marrow is seen in approximately 50% of patients at presentation. [2] Although it is a very aggressive neoplasm with a poor prognosis, there have been reports showing an indolent course or a rapid response to treatment and more promising course. [3] We describe a woman who is diagnosed as cutaneous CD4+/CD56+ HN, without systemic involvement.
Case Report
A 38-year-old woman referred with an asymptomatic nodule on the right cheek. She had noticed a small erythematous papule two months ago, which enlarged rapidly. Her past medical and family history was noncontributory. Physical examination was normal and peripheral lymph nodes were not palpable. Dermatological examination showed 2 × 2.5 cm, erythematous, round, nontender, crusty nodule on the right cheek [Figure - 1]. On biopsy, the dermis was infiltrated with medium sized, blastlike lymphocytes with large round nuclei [Figure - 2]. Immunophenotypic evaluation showed positivity for CD4 and CD56 and negativity for CD3, CD20, Tdt, myeloperoxidase, pancytokeratin ve Ki67 [Figure - 3] and [Figure - 4]. T cell gene rearrangement could not be performed. PCR examination for EBV was negative. Routine laboratory investigations were within normal ranges. Peripheral blood analysis, bone marrow biopsy, chest X-ray and computerized tomography (CT) of the thorax, abdomen, cranium and paranasal sinuses showed no abnormalities. Based on these findings, she was diagnosed as cutaneous CD4+/CD56+ HN without systemic involvement. The patient was started on chemotherapy consisting of cyclophosphamide, adriamycin, vincristine and prednisolone. Complete remission was noted at the end of third regimen. She received three cycles of chemotherapy and no recurrence was observed over the following one year.
 |
| Figure 1 :Erythematous, round, crusty nodule on the right cheek |
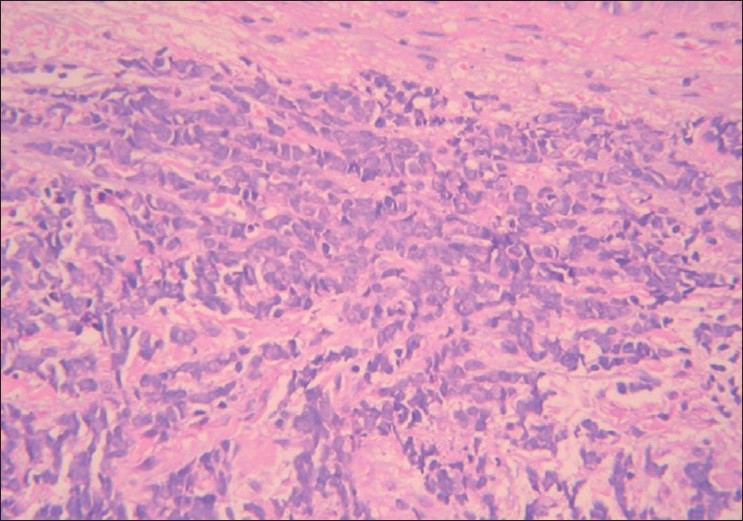 |
| Figure 2 :Blastoid appearance of lymphocytes with large round nucleus. (H and E, ×200) |
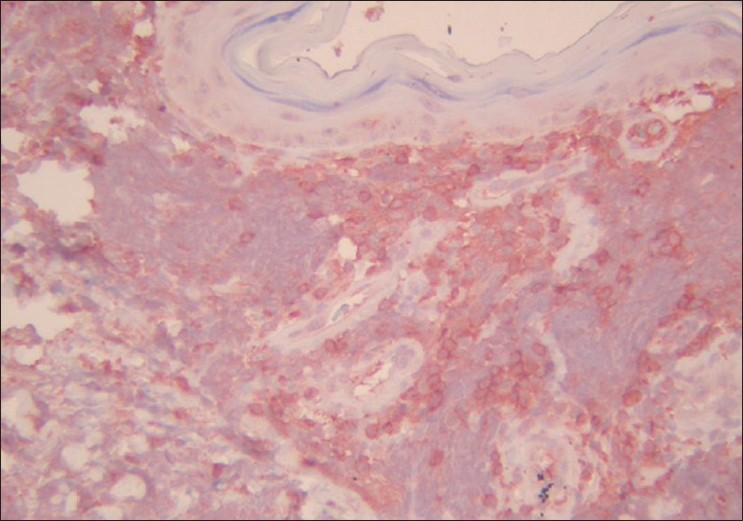 |
| Figure 3 :CD4 positivity in blast-like cells (AntiCD4 ×200) |
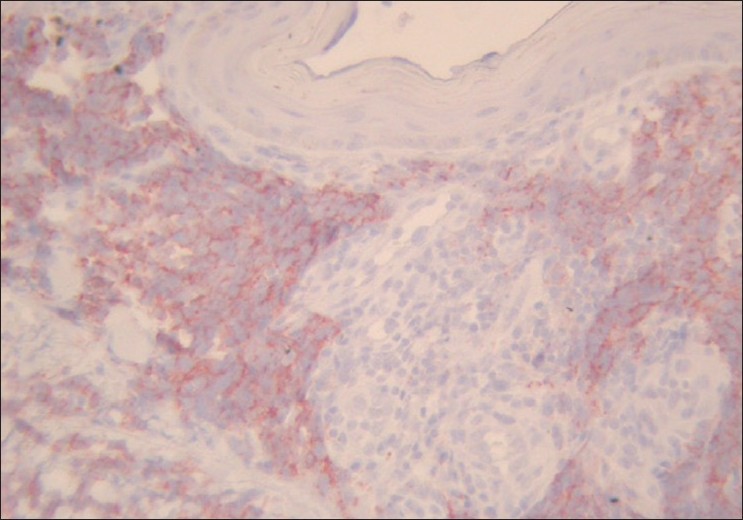 |
| Figure 4 :CD56 positivity in blast-like cells |
Discussion
CD4+/CD56+ hematodermic neoplasm (HN) is a rare form of cutaneous malignant lymphoma. In the WHO-EORTC classification of cutaneous lymphomas with primary cutaneous manifestations, this neoplasm has been included as a distinct clinicopathological entity under precursor hematological neoplasms. [2] Although believed to arise from committed NK progenitor cells, recent studies argue against an NK cell origin and lymphoid related plasmacytoid dendritic cell, as indicated by the expression of the interleukin-3 receptor alpha subunit (CD123) and blood dendritic cell antigen2 (BDCA2) [1],[2],[3],[4],[5],[6]
The disease has a propensity for extranodal sites such as the skin, soft tissues and mediastinium with dissemination to lymph nodes and bone marrow. Controversially to our patient, rapid extracutaneous dissemination usually occurs. The mechanism of this tropism to involve the skin is not well understood. [5]
CD4+/CD56+ HN accounts for 0.07% of all cutaneous lymphomas. [6] Patients are mostly elderly adults although cases in younger individuals, including small children, have been reported. [5] There is a predominance of males. [1] On the basis of published data, over 90% of CD4+/CD56+ HN cases manifested with cutaneous lesions. [1],[2],[3],[4],[5],[6] The dermatologic manifestations are diverse. Usually, as in our patient, lesions are solitary or localized at the onset of disease, then eventually spread with time and may include erythema, patches, papules, nodules, ulcers and bruise like lesions. In patients with primary cutaneous disease, the time interval between the onset of skin lesions and leukemic spread varies usually between a few weeks and several months. In one exceptional case, there was a 15-year history of multiple cutaneous lesion. [7] In our patient, we did not detect systemic involvement for one year.
Diagnosis is made histopathologically. It is characterized by a nonepidermotropic, diffuse monomorphous infiltrate of medium sized neoplastic cells with a blastoid morphology, as in our patient. Reactions like angiocentricity, angiodestruction and necrosis are uncommon. In most cases, immunophenotypes are CD2±, CD3-, CD4±, CD5, CD7±, CD56+, CD123+, CD68-and terminal deoxynucleotidyl transferase (TdT), T-cell intracellular antigen-1(TIA-1). [1],[3],[6] Histologic differential diagnoses include lymphoblastic, myeloblastic and especially extranodal NK/T cell neoplasms and leukemia cutis. It can be differentiated from leukemia cutis by negative myeloid markers such as myeloperoxidase, lysozyme, CD13, CD15 and T-cellineaage markers such as TIA1. [8] Extranodal NK/T cell lymphoma usually presents in male adults as plaques and tumors with a predilection for the trunk and extremities. Prominent angiocentricity with accompanying necrosis is a characteristic histological finding. Extranodal NK/T cell lymphoma is usually EBV+ and the neoplastic cells express CD2, CD56, TIA1, granzyme B and perforin, but lack surface CD3. [1],[9]
CD4+/CD56+ HN follow an aggressive clinical course and prognosis is poor. Patients with this type of lymphoma usually survive for one year; only exceptional cases have longer survivals. [8] The median survival was only 14 months, and two and five year overall survivals have been reported with percentages of 33 and 6%, respectively. [10]
In conclusion, CD4+/CD56+ HN is a rare and uncommon form of cutaneous lymphoma. Because of its aggressive behavior, it is important to diagnose it accurately for proper clinical management.
| 1. |
Cerroni L, Gatter K, Kerl H. An illustrated guide to skin lymphoma. Odder; 2004:131-7.
[Google Scholar]
|
| 2. |
Willemze R, Jaffe ES, Burg G, Cerroni L, Berti E, Swerdlow SH, et al. WHO-EORTC classification for cutaneous lymphomas. Blood 2005;105:3768-85
[Google Scholar]
|
| 3. |
3 Chang SE, Choi HJ, Huh J, Choi JH, Moon KC, Koh JK. A case of cutaneous blastic NK lymphoma in a 32-year-old Korean woman. Int J Dermatol 2006;45:591-3
[Google Scholar]
|
| 4. |
Chaperot L, Bendriss N, Manches O, Gressin R, Maynadie M, Trimoreau F, et al. Identification of a leukemic counterpart of the plasmacytoid dendritic cells. Blood 2001;97:3210-7.
[Google Scholar]
|
| 5. |
Eguaras AV, Lo RW, Veloso JD, Tan VG, Enriquez ML, Del Rosario ML. CD4+/CD56+ hematodermic neoplasm: blastic NK cell lymphoma in a 6-year-old child: report of a case and review of literature. J Pediatr Hematol Oncol 2007;29:766-9
[Google Scholar]
|
| 6. |
Petrella T, Bagot M, Willemze R, Beylot-Barry M, Vergier B, Delaunay M, et al. Blastic NK-cell lymphomas (agranular CD4+CD56+ hematodermic neoplasms): a review. Am J Clin Pathol 2005;123:662-75.
[Google Scholar]
|
| 7. |
Brody JP, Allen S, Schulman P, Sun T, Chan WC, Friedman HD, et al. Acute agranular CD4-positive natural killer cell leukemia. Comprehensive clinicopathologic studies including virologic and in vitro culture with inducing agents. Cancer 1995;15:75:2474-83.
[Google Scholar]
|
| 8. |
Hsu Mei-Yu, Murphy GF. Cutaneous Lymphomas and Leukemias. Elder DE, editor. 6th ed. Philadeilphia: Lever's Histopathology of the Skin; 2009. P. 959-60
[Google Scholar]
|
| 9. |
Cibull TL, Thomas AB, O'Malley DP, Billings SD. CD4+ CD56+ hematodermic neoplasm. Am J Dermatopathol 2007;29:59-61.
[Google Scholar]
|
| 10. |
Bekkenk MW, Jansen PM, Meijer CJ, Willemze R. CD56+ hematological neoplasms presenting in the skin: a retrospective analysis of 23 new cases and 130 cases from the literature. Ann Oncol 2004;15:1097-108
[Google Scholar]
|
Fulltext Views
2,763
PDF downloads
2,768





![[Figure - 1]](#fig_ijdvl_2010_76_6_723_72471_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2010_76_6_723_72471_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2010_76_6_723_72471_f3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2010_76_6_723_72471_f4.jpg){kind=link}