Translate this page into:
Cutaneous mercury granuloma following accidental occupational exposure
2 Department of Pathology, Christian Medical College, Ludhiana, Punjab, India
3 Department of Surgery, Christian Medical College, Ludhiana, Punjab, India
Correspondence Address:
Anisha George
Department of Dermatology, Christian Medical College, Ludhiana - 141 008, Punjab
India
| How to cite this article: George A, Kwatra KS, Chandra S. Cutaneous mercury granuloma following accidental occupational exposure. Indian J Dermatol Venereol Leprol 2015;81:57-59 |
Sir,
Inorganic mercury exists as a liquid metal at room temperature. This silver-colored substance is still routinely used in India in thermometers and sphygmomanometers. Exposure to metallic mercury can have local as well as potentially serious systemic effects. We report a case of accidental occupational exposure, which highlights the need to use alternatives to mercury thermometers.
A 28-year-old hospital staff nurse presented with complaints of redness, itching and swelling over the dorsum of her left hand 12 days after accidental injury from a mercury thermometer. The lesion had been progressively increasing in size since the injury. There was no history of abdominal pain, nausea, vomiting, diarrhea, breathlessness, cough, decreased urine output, visual disturbances or changes in affect.
Cutaneous examination revealed a curvilinear, pink, fleshy plaque with surrounding edema over the left third knuckle [Figure - 1]. She was initially treated with potent topical steroids for 2 days, after which an excision biopsy was performed (2 weeks after the injury). Histopathologic examination revealed a dense lympho-histiocytic infiltrate in the dermis, centered around blood vessels and sweat glands. Also visualized in the deep dermis were black opaque globules indicative of mercury, surrounded by a foreign body granulomatous reaction [[Figure - 2] and [Figure - 3]]. No polarizable material suggestive of glass fragments was detected. The overlying epidermis showed hyperkeratosis and mild acanthosis.
 |
| Figure 1: Curvilinear, faintly erythematous plaque with surrounding edema over the dorsum of left hand |
 |
| Figure 2: The covering epidermis shows hyperkeratosis and mild acanthosis. The dermis shows a dense lympho-histiocytic infiltrate around blood vessels and sweat glands. Black mercury pigment is visible in the deep dermis (red arrows). (H and E, ×40) |
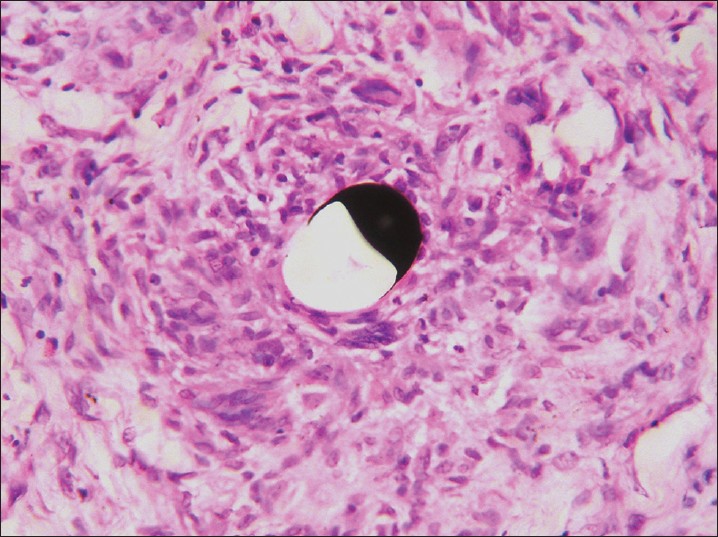 |
| Figure 3: High power view showing dark spherical mercury pigment surrounded by a granulomatous reaction with multinucleated giant cells. (H and E, ×400) |
Following the excision, the swelling and irritation subsided. The patient did not develop any systemic or psychiatric symptoms. Blood mercury levels were not measured.
Accidental inoculation of metallic mercury can have local as well as systemic effects. Local cutaneous reactions include erythema, indurated nodules and plaques with or without ulceration. [1] Gradual absorption from the inoculation site can lead to systemic mercury poisoning. Slow oxidization of metallic mercury to mercury salts occurs on contact with tissue, which then rapidly get distributed systemically and inhibit thiol-containing enzymes. [2] Oral ingestion of inorganic mercury salts or inhalation of mercury vapors can also lead to systemic mercury poisoning. Systemic effects include acute respiratory failure, renal failure, neurologic features and psychiatric problems. [1] Rarely, systemic contact dermatitis (baboon syndrome) following mercury exposure in previously sensitized individuals can also occur. [3]
Metallic mercury, on histopathology, is seen as dark, opaque, spherical globules. [4] Histologically, early reactions show acute inflammation, necrosis and abscess formation with or without ulceration of the overlying skin. Late reactions show granuloma formation with foreign body giant cells around the mercury deposits, perivascular lymphocytic infiltrates, fibrosis and fat necrosis. [5] Our patient had a late granulomatous reaction.
Management of mercury inoculation includes prompt and complete surgical excision to halt local reaction and systemic absorption. Blood and urine levels of mercury should be monitored where available, and regular assessment for systemic signs and symptoms of mercury poisoning should be done, including evaluation for neuropsychiatric manifestations. [5] Blood and urine levels indicate mercury exposure but do not correlate well with toxicity. [2] Systemic toxicity can be treated with dimercaprol, d-penicillamine or meso-2,3-dimercaptosuccinic acid. [6] Hemodialysis with or without l-cysteine as a chelating agent can be used in patients with acute renal failure.
Since mercury thermometers carry the hazard of accidental inoculation and systemic toxicity, digital thermometers have been recommended as an alternative, which also have the added advantage of being more accurate. [7] The mercury-free hybrid blood pressure monitor also seems to be a reliable alternative to the currently used mercury sphygmomanometers, with the same level of accuracy. [8] Hospitals could therefore switch over to mercury-free gadgets to prevent accidental exposure to mercury. We also recommend that the mercury-containing devices currently in use be disposed of in an environment-friendly manner. [9]
| 1. |
Jun JB, Min PK, Kim DW, Chung SL, Lee KH. Cutaneous nodular reaction to oral mercury. J Am Acad Dermatol 1997;37:131-3.
[Google Scholar]
|
| 2. |
Altmeyer MD, Burgdorf MR, Newsome RE, Wang AR. Cutaneous mercury granuloma: A case report. Cutis 2011;88:189-93.
[Google Scholar]
|
| 3. |
Wen L, Yin J, Ma D-L, Lanier B. Baboon syndrome induced by mercury - first case report in China. Contact Dermatitis 2007;56:356-7.
[Google Scholar]
|
| 4. |
Lupton GP, Kao GF, Johnson FB, Graham JH, Helwig EB. Cutaneous mercury granuloma: A clinicopathologic study and review of the literature. J Am Acad Dermatol 1985;12:296-303.
[Google Scholar]
|
| 5. |
Ellabban MG, Ali R, Hart NB. Subcutaneous metallic mercury injection of the hand. Br J Plast Surg 2003;56:47-9.
[Google Scholar]
|
| 6. |
Graeme KA, Pollack CV Jr. Heavy metal toxicity, Part I: Arsenic and mercury. J Emerg Med 1998;16:45-56.
[Google Scholar]
|
| 7. |
Fadzil FM, Choon D, Arumugam K. A comparative study on the accuracy of noninvasive thermometers. Aust Fam Physician 2010;39:237-9.
[Google Scholar]
|
| 8. |
Stergiou GS, Karpettas N, Kollias A, Destounis A, Tzamouranis D. A perfect replacement for the mercury sphygmomanometer: The case of the hybrid blood pressure monitor. J Hum Hypertens 2012;26:220-7.
[Google Scholar]
|
| 9. |
DiCarlo M, Ruck B, Marcus S. How should a fever mercury thermometer be disposed of? A survey of those likely to be asked. Pediatrics 2002;109:E71-1.
[Google Scholar]
|
Fulltext Views
3,495
PDF downloads
2,302





![[Figure - 1]](#fig_ijdvl_2015_81_1_57_148574_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2015_81_1_57_148574_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2015_81_1_57_148574_f3.jpg){kind=link}