Translate this page into:
Cutaneous metastasis from urologic tumors
Correspondence Address:
Prabhash Kumar
Room No. 6, Department of Medical Oncology, Tata Memorial Hospital, Parel, Mumbai 400 012, Maharashtra
India
| How to cite this article: Kumar P, Prasad N, Biswas G, Parikh P M. Cutaneous metastasis from urologic tumors. Indian J Dermatol Venereol Leprol 2006;72:86 |
 |
|
 |
|
Sir,
Metastasis from urological tumors is common, but skin metastasis is uncommon. It is important to keep skin metastasis as a differential diagnosis in cases of primary urological tumors because it helps in the diagnosis, staging, and proper treatment. Here, we report on two cases that illustrate these issues.
CASE 1
A 55-year-old man presented with hematuria for 2 weeks. Systemic examination was normal. Cystoscopy revealed a proliferative lesion in the lateral wall of the urinary bladder. Histopathology revealed a muscle invasive grade-II transitional cell carcinoma. CT scan of the abdomen and pelvis showed a mass in the lateral wall of the urinary bladder and pelvic lymphadenopathy.
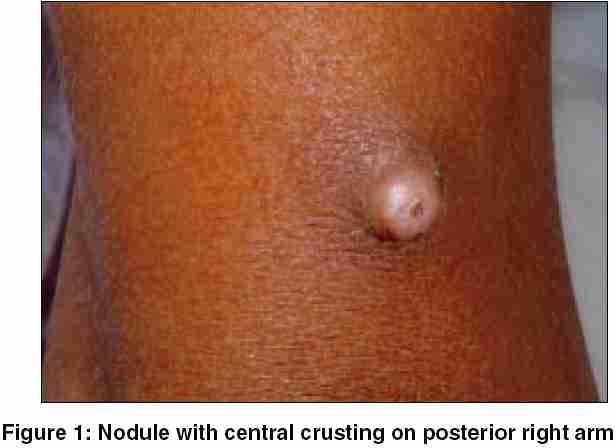
Neoadjuvant chemotherapy was planned and he was started on 1200 mg/m2 gemcitabine and 80 mg/m2 cisplatin every 3 weeks. Re-evaluation with a CT scan of the abdomen and pelvis after three cycles of chemotherapy showed regression of the lesion. At the same time he developed a nodular swelling on the right arm. On examination, it was a slightly reddish, smooth-surfaced nodule, 1-1.5 cm in size, with central crusting on the lower half of the right arm. It was firm-to-hard, nontender, and nonadherent to the underlying structures [Figure - 1]. Fine-needle aspiration cytology (FNAC) was suggestive of a metastatic carcinoma from the urinary bladder [Figure - 2]. He was offered second-line chemotherapy but the patient refused further chemotherapy.
CASE 2
A 49-year-old man presented with abdominal pain and swelling in the left postauricular area for 4 months. CT scan of the abdomen showed a mass in the left kidney extending outside the capsule with thrombosis in the inferior vena cava. Subsequently, a trucut biopsy was done and was reported as renal cell carcinoma. He was then referred to our hospital for further management.
Examination revealed a purple, smooth-surfaced, nontender nodule, 3-4 cm in size, behind the left ear. It was fixed to the underlying structures and mimicked a cutaneous hemangioma. FNAC of the lesion showed a metastatic carcinoma from the kidney. The patient was given three cycles of chemotherapy with vinblastine but did not respond to it.
DISCUSSION
Urologic tumors most commonly metastasize to the regional lymph nodes, liver, lung, and bone. Apart from a drug eruption and opportunistic infections, the differential diagnosis of an eruption in patients with a genitourinary cancer should include cutaneous metastasis because, though rare (the incidence for urologic tumors is 0.73%),[1] a delay in the diagnosis is common and leads to ineffective treatment. Skin metastasis is usually associated with advanced disease and sometimes it may be the initial sign of visceral dissemination as seen in both the cases presented here.[2] The skin lesions helped in confirming the progression of disease in one of our patients and the metastatic nature of the disease in the other.
The commonest sites of metastasis from renal cell carcinoma are the scalp and face, but for urinary tract malignancies it is the abdominal skin.[1],[3] Most patients have at least one other systemic site of metastasis but in both our patients the skin was the only site. The most common manifestation of cutaneous metastasis is urticaria and a nonspecific rash, but patients can present with nodular and papular lesions. One of our patients had a nodule surmounted by a pustule, whereas the other one had a purple nodule resembling a cutaneous hemangioma.[1]
Histologically, cutaneous metastasis predominantly involves the dermis. Metastatic lesions often preserve histologic similarities with the primary lesion. The prognosis of patients with skin metastasis from urologic tumors is poor; they usually die within 6 months of diagnosis. Patients with cutaneous metastasis are usually treated with a palliative intent, but rarely surgical excision, radiotherapy, or both are utilized.[4]
These cases are being presented for their rarity and to emphasize that skin metastasis should be considered in the differential diagnosis of skin lesions in patients with a urological tumor.
| 1. |
Thomas JM, Hong Wu, Richard EG, Gary H, Neil T, Lessin SR, et al . Cutaneous metastases from genitourinary malignancies. Urology 2004;63:1021-6.
[Google Scholar]
|
| 2. |
Reingold IM. Cutaneous metastases from internal carcinoma. Cancer 1966;19:162-8.
[Google Scholar]
|
| 3. |
Dorairajan LN, Hemal AK, Aron M, Rajeev TP, Nair M, Seth A, et al . Cutaneous metastases in renal cell carcinoma. Urol Int 1999;63:164-7.
[Google Scholar]
|
| 4. |
Brownstein MH, Helwig EB. Spread of tumors to skin. Arch Dermatol 1973;107:80-6.
[Google Scholar]
|
Fulltext Views
2,191
PDF downloads
929





![[Figure - 1]](#fig_ijdvl_2006_72_1_86_19737_1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2006_72_1_86_19737_2.jpg){kind=link}