Translate this page into:
Cutaneous metastasis of an advanced prostate cancer
Correspondence Address:
Mohammad Abid Keen
Iqbal Abad, KP Road, Near Masjid Usman, Anantnag - 192 101, Kashmir
India
| How to cite this article: Keen MA, Hassan I. Cutaneous metastasis of an advanced prostate cancer. Indian J Dermatol Venereol Leprol 2013;79:828-829 |
Sir,
Primary visceral malignancies uncommonly present with skin involvement with a reported incidence between 2% and 9% and their presence is indicative of an advanced disease and poor prognosis. The most common tumors to metastasize to skin are breast, lung, colorectal, renal and ovarian carcinomas. [1] Despite the high incidence of prostatic cancer, cutaneous and subcutaneous metastases of this cancer are extremely rare, seen in <1% cases. We report a case of an elderly male with carcinoma of the prostate with multiple cutaneous metastases.
A 70-year-old man presented with 1 month history of multiple skin colored to erythematous papulonodular lesions variable in size over the pubic region and inner aspects of thigh. These lesions first appeared over the suprapubic area and progressively increased in size and involved inner aspects of thighs and left inguinal region. These lesions were associated with discomfort, but were not associated with ulceration and bleeding. About a year back, he had presented to the emergency department with urinary retention. He was diagnosed to have carcinoma of the prostate and his prostate-specific antigen (PSA) level was found to be 210 ng/ml.
Transrectal ultrasound guided biopsy was carried out, which revealed poorly differentiated prostatic adenocarcinoma with a Gleason score of 9 in all the 8 core biopsies performed. There was no perineural invasion or extraglandular extension. A staging bone scan was performed at the time of diagnosis, which did not show any evidence of bony involvement.
Patient underwent a complete androgen blockade with Buserelin and Cyproterone acetate. Almost 1 year after the diagnosis, patient noted development of cutaneous lesions at the pubic region. These lesions were considered to be cutaneous metastases from the prostatic cancer. Patient also complained of multiple bone pains, loss of weight and appetite. Repeat bone scan revealed multiple metastatic lesions of pelvic bones.
Cutaneous examination revealed multiple erythematous dome shaped papueonodular lesions, with a smooth shiny surface, varying in size from 5 mm to 1 cm presenting over the suprapubic region, left inguinal region and inner aspect of left thigh [Figure - 1]. These lesions were non-tender, firm in consistency and fixed to the overlying skin, but not to the underlying structures. Scrotum was normal, but penis was thick, edematous infiltrated and deformed in shape. Rest of the mucocutaneous examination was unremarkable. Systemic examination of the patient was also normal.
 |
| Figure 1: Multiple erythematous dome shaped papulonodular lesions, ranging in size from 5 mm to 1 cm |
Routine investigations showed a hemoglobin of 7.8 g/dl and increased liver enzymes (serum glutamic oxaloacetic transaminase and serum glutamic pyruvic transaminase). Fine needle aspiration cytology revealed adenocarcinomatous cells of uncertain origin. Excisional biopsy of one of the papules revealed stratified squamous epidermis on the surface, with rows and prostate acini-like glandular structures appearing due to the ectatic lymphatic spaces due to the lymphangiectasia secondary to metastasis blocking lymphatics [Figure - 2]. PSA level was also elevated.
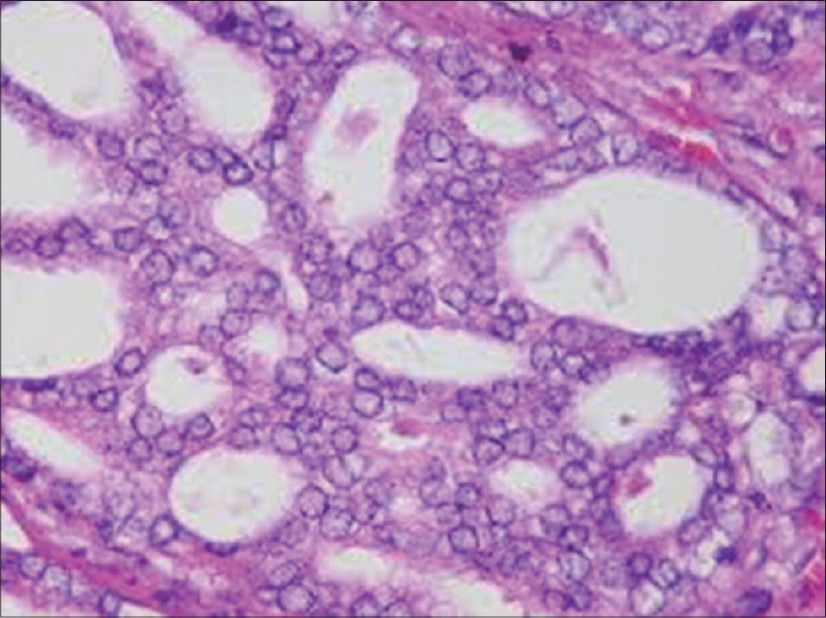 |
| Figure 2: Histopathological image of one of the papules revealing prostate acini-like glandular structures appearing due to ectatic lymphatic spaces due to lymphangiectasia secondary to metastasis blocking lymphatics (H and E, ×40) |
Radiographs of pelvis revealed diffuse osteosclerotic lesions. Chest radiograph as well as ultrasound abdomen were normal. Patient was subjected to palliative care with radiotherapy to the pelvic bones.
Cutaneous metastases from internal malignancies are relatively rare, seen in about 2-9% of malignancies. [2] Cutaneous metastases occur more commonly with mammary, pulmonary, renal and colonic cancers and are seen in the advanced stage of malignancy, associated with a poor prognosis. Although carcinoma of the prostate is common, it is responsible for lesser than 1% of cutaneous metastases.
Cutaneous metastases from prostatic carcinoma are usually asymptomatic and may occur at single or multiple sites. [3] The most common sites involved are the lower abdomen, genitalia and thighs. [4] Metastatic lesions are usually papules and nodules and they rarely ulcerate. They may have a zosteriform distribution or may appear as sclerodermoid lesions. Other rare manifestations include priapism, penile metastasis, gynecomastia and breast metastasis. Skin metastases from prostatic cancer are an ominous finding and most of the patients die within 6 months.
Although the mechanism of cutaneous involvement is not well-understood, suggested routes include embolization of vessels, dissemination through lymphatics and through perineural lymphatics.
Immunohistochemistry is an important tool in establishing organ of origin when histology is not conclusive. [5] A large majority of metastatic adenocarcinomas are P501S positive (99%). A small subset of metastatic prostatic adenocarcinoma shows significant differences in staining intensity and extent of PSA and P501S and therefore combined use of these markers may result in increased sensitivity for detecting prostatic origin. [6] Cutaneous metastases from a prostatic carcinoma signifies an advanced stage, aggressive behavior and a grave prognosis, with disease specific survival lesser than 6 months. Thus, the treatment at this stage is palliative care, which includes keeping the lesions dry and clean. Debridement is a good option for bleeding or crusting lesions.
| 1. |
Krathen RA, Orengo IF, Rosen T. Cutaneous metastasis: A meta-analysis of data. South Med J 2003;96:164-7.
[Google Scholar]
|
| 2. |
Spencer PS, Helm TN. Skin metastases in cancer patients. Cutis 1987;39:119-21.
[Google Scholar]
|
| 3. |
Steinkraus V, Lange T, Abeck D, Mensing H, Ring J. Cutaneous metastases from carcinoma of the prostate. J Am Acad Dermatol 1995;32:665-6.
[Google Scholar]
|
| 4. |
Jones C, Rosen T. Multiple red nodules on lower abdomen. Metastatic carcinoma of the prostate. Arch Dermatol 1992;128:1532, 1535.
[Google Scholar]
|
| 5. |
Saeed S, Keehn CA, Morgan MB. Cutaneous metastasis: A clinical, pathological, and immunohistochemical appraisal. J Cutan Pathol 2004;31:419-30.
[Google Scholar]
|
| 6. |
Sheridan T, Herawi M, Epstein JI, Illei PB. The role of P501S and PSA in the diagnosis of metastatic adenocarcinoma of the prostate. Am J Surg Pathol 2007;31:1351-5.
[Google Scholar]
|
Fulltext Views
6,963
PDF downloads
2,300





![[Figure - 1]](#fig_ijdvl_2013_79_6_828_120745_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2013_79_6_828_120745_f2.jpg){kind=link}