Translate this page into:
Cutaneous sarcoidosis and macular amyloidosis occurring at the same site
Correspondence Address:
Sanchita Karmakar
Department of Dermatology and STD, Vardhman Mahavir Medical College and Safdarjung Hospital, New Delhi - 110 029
India
| How to cite this article: Karmakar S, Ramesh V. Cutaneous sarcoidosis and macular amyloidosis occurring at the same site. Indian J Dermatol Venereol Leprol 2016;82:574-576 |
Sir,
Sarcoidosis is a multisystem disorder of unknown etiology histologically characterized by non-caseating epithelioid cell granulomas. Primary localized cutaneous amyloidosis shows deposition of amyloid in apparently normal skin with no evidence of systemic amyloidosis. The association of systemic sarcoidosis and amyloidosis has been reported.[1],[2],[3] However, the association of macular amyloidosis, a clinical subtype of primary localized cutaneous amyloidosis with cutaneous sarcoidosis is rare.[4]
A 54-year-old woman presented with a history of hyperpigmentation of the skin of her upper back and the extensor aspect of her forearms for 7–8 months. The pigmentation started with a burning sensation followed by the development of raised skin colored lesions over 3–4 months. There were similar lesions on the shins. Clinical examination revealed multiple, skin - colored, discrete papules and plaques on a background of hyperpigmentation on the sun exposed areas of the upper back and the extensor aspects of forearms. The skin underlying and surrounding these lesions showed rippled pigmentation [Figure - 1]a and [Figure - 1]b. Similar lesions were present on the shins. In addition, three, discrete, dull red, 1 cm × 1 cm papules were present on the chest. Systemic examination was non-contributory. Skin biopsy from hyperpigmentation of the upper back showed homogeneous, eosinophilic amyloid deposits in the papillary dermis [Figure - 2]. Biopsy from a papular lesion with underlying pigmentation showed naked epithelioid cell granulomas and giant cells with a few lymphocytes in the superficial and mid-dermis, within the areas where amyloid was deposited. Melanophages were also seen in the papillary dermis [Figure - 3]. The presence of the amyloid material was confirmed by Congo red stain.
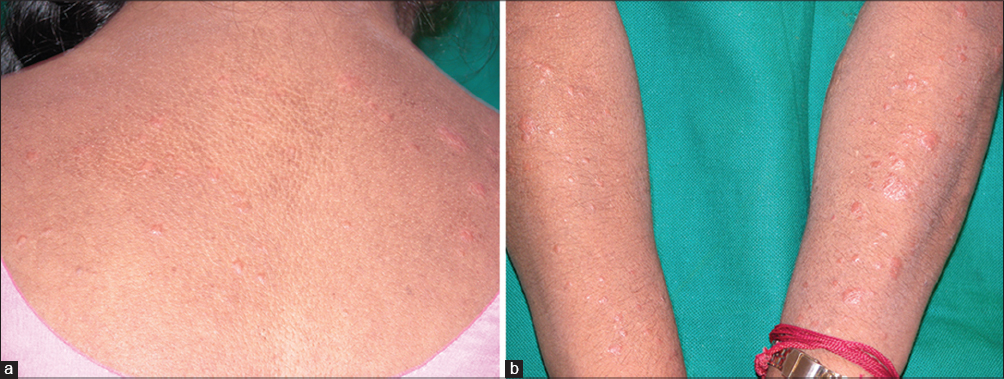 |
| Figure 1: Rippled pigmentation with skin colored papules on the (a) back and (b) forearms |
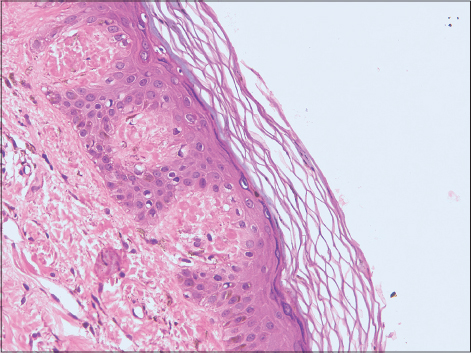 |
| Figure 2: Amorphous amyloid deposits in papillary dermis (H and E, ×400) |
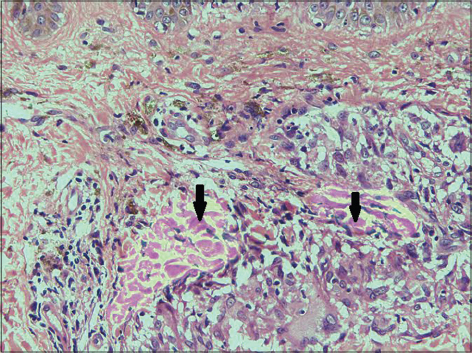 |
| Figure 3: Sarcoidal granuloma surrounded by homogeneous amyloid deposits (H and E, ×200) |
Based on the above findings, the diagnosis of cutaneous sarcoidosis and cutaneous amyloidosis occurring at the same location was made. Complete hemogram, serum calcium, angiotensin converting enzyme levels and 24 h urine calcium levels were within normal limits. Mantoux test (with 5 units of PPD) was positive. Chest X-ray and electrocardiogram were normal. Pulmonary function test showed mild restriction of forced vital capacity.
Among the three known subtypes of primary localized cutaneous amyloidosis, macular and lichenoid are the most common presentations. The histopathology of macular amyloidosis typically reveals deposition of globular, amorphous eosinophilic material within the dermal papillae. Scattered apoptotic keratinocytes are also seen and this is believed to be the source of the amyloid material which reacts with anti-keratin antibody.[4] The etiopathogenesis of this amyloid deposition remains unknown though fibrillar body theory and secretory theory have been proposed.
The exact etiopathogenesis of cutaneous sarcoidosis occurring in the same area as cutaneous amyloidosis is not clear. However, apoptotic keratinocytes often seen in macular amyloidosis may provide cutaneous dendritic cells with a rich source of autoantigens to initiate an autoimmune responses.[5] The occurrence of a sarcoid granuloma at the site of macular amyloidosis is likely to be an autoimmune response, or this could be a coincidental association of the two diseases.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Schade L, Carmes ER, de Barros JA. Mediastinal lymph node amyloidosis in a patient with sarcoidosis. J Bras Pneumol 2007; 33:222-5.
[Google Scholar]
|
| 2. |
James DG, Sharma OP. Overlap syndromes with sarcoidosis. Postgrad Med J 1985; 61:769-71.
[Google Scholar]
|
| 3. |
Nakai N, Ozawa A, Katoh N. Nodular primary localized cutaneous amyloidosis in a patient with pulmonary sarcoidosis. Indian J Dermatol 2014;59:307-8.
[Google Scholar]
|
| 4. |
Dahdah MJ, Kurban M, Kibbi AG, Ghosn S. Primary localized cutaneous amyloidosis: A sign of immune dysregulation? Int J Dermatol 2009;48:419-21.
[Google Scholar]
|
| 5. |
Udey MC. Skin dendritic cells in immunity and autoimmunity. J Investig Dermatol Symp Proc 2004;9:15-7.
[Google Scholar]
|
Fulltext Views
3,157
PDF downloads
1,501





![[Figure - 1]](#fig_ijdvl_2016_82_5_574_183627_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2016_82_5_574_183627_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2016_82_5_574_183627_f3.jpg){kind=link}