Translate this page into:
Cutis laxa-like pseudoxanthoma elasticum with osteoma cutis
2 Department of Dermatology, Public Hospital in Kelkit, Gumushane, Turkey
3 Department of Ophthalmology, Istanbul Education and Research Hospital, Istanbul, Turkey
4 Department of Pathology, Acıbadem University School of Medicine, Istanbul, Turkey
Correspondence Address:
Cem Leblebici
Department of Pathology, Org. Nafiz Gurman Street Istanbul Education and Research Hospital, Istanbul
Turkey
| How to cite this article: Leblebici C, Falay T, Zırtıloğlu S, Demirkesen C. Cutis laxa-like pseudoxanthoma elasticum with osteoma cutis. Indian J Dermatol Venereol Leprol 2017;83:464-467 |
Sir,
Pseudoxanthoma elasticum is a rare inherited multisystem disease, characterized by degenerative changes and calcification of the elastic fibers in the mid dermis, the blood vessels and Bruch's membrane of the eye. Typical cutaneous lesions are characterized by yellow papules and preferentially involve the flexural regions. The lesions may be accompanied by skin laxity in cases with extensive involvement, resulting in redundant folds and simulating cutis laxa.[1],[2],[3],[4] Herein, we report a case of cutis laxa-like pseudoxanthoma elasticum associated with cutaneous ossification, namely, osteoma cutis.
A 40-year-old woman presented with wrinkled, loose, pendulous skin and pigmented patches. The patient noticed the changes on the neck and chest ten years ago and lesions gradually extended to the trunk, thighs and arms. When the patient was admitted to a dermatology clinic 7 years ago, she was diagnosed as acquired cutis laxa due to syphilis as no other underlying condition was found associated with cutis laxa, except the positive results for venereal diseases research laboratory test, Treponema pallidum hemagglutination test and fluorescent treponemal antibody absorption test. Then, she received three doses of penicillin treatment.
The patient consulted the dermatology clinic of Istanbul Education and Research Hospital because her lesions were gradually extending and also there were brown spots on her body. Dermatological examination revealed marked wrinkling on the neck, trunk, abdomen and axillae together with loose and redundant skin, especially on the arms and abdomen [Figure - 1] and [Figure - 2]. Multiple purplish brown round to oval plaques 1–3 cm in size with irregular borders on the neck, abdomen, trunk, arms and thighs were observed. Brown reticulated patches on the chest and yellowish papules 3–4 mm in size on both sides of the neck and the vermilion border of the lip were noted [Figure - 3] and [Figure - 4]. The skin lesions were asymptomatic. There was no significant family history of similar skin lesions. In the differential diagnosis, we considered cutis laxa, pseudoxanthoma elasticum and pseudoxanthoma elasticum-like syndrome.
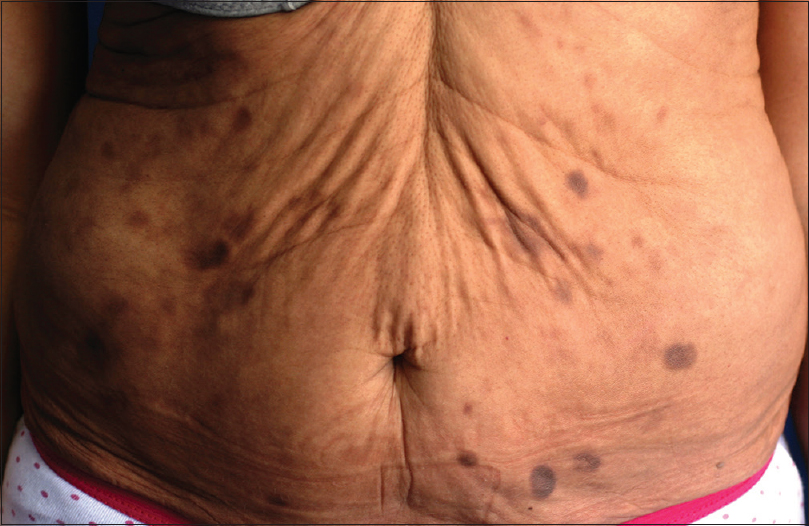 |
| Figure 1: Loose, pendulous skin with redundant folds and multiple purplish brown round to oval plaques 1–3 cm in size with irregular borders on the abdomen |
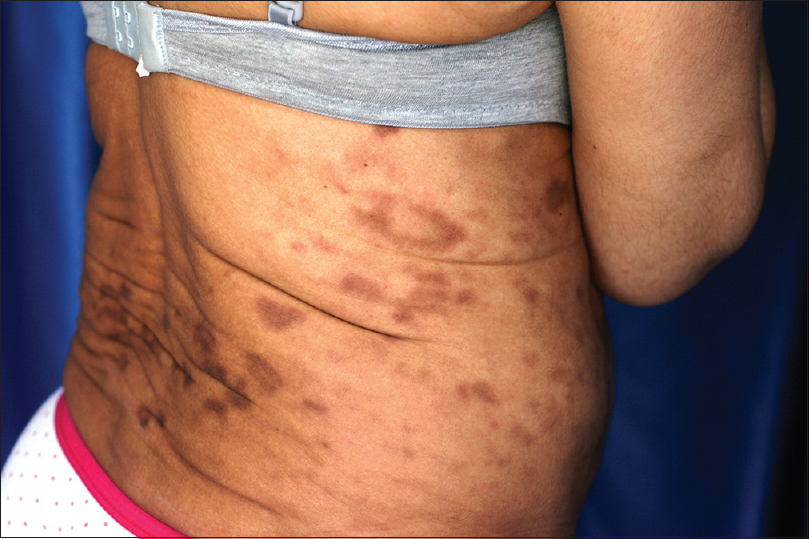 |
| Figure 2: Brown plaques with irregular borders on the trunk |
 |
| Figure 3: Yellowish coalescing papules 3–4 mm in size on the neck |
 |
| Figure 4: Yellowish papules on the vermilion border of the lip |
The laboratory tests which included complete blood cell count, liver function test, urinalysis, serum calcium, phosphorus, thyroid function test, complement 3, complement 4, erythrocyte sedimentation rate, protein immunoelectrophoresis, prothrombin time, activated partial thromboplastin time and factors VII, VIII, IX were within normal limits. Serological investigation showed positive result for only T. pallidum hemagglutination test with titers of 1:1280. We were unable to find any previous report of the association between syphilis and pseudoxanthoma elasticum. Other serological markers of Borrelia and human immunodeficiency virus infection were negative. Chest and abdominal X-ray films and electrocardiogram showed no abnormalities. Fundoscopic examination showed bilateral angioid streaks and a juxtafoveal hyperpigmented scar from previous subretinal membrane rupture in the left eye [Figure - 5]. Her vision acuity was 6/6. Her blood pressure was 200/100 mmHg. She was not using antihypertensive drugs. Valsartan, an angiotensin II receptor antagonist, was started orally at a dose of 80 mg/day. Echocardiography showed left ventricular hypertrophy and left ventricular systolic dysfunction. Abdominopelvic ultrasonography was within normal limits.
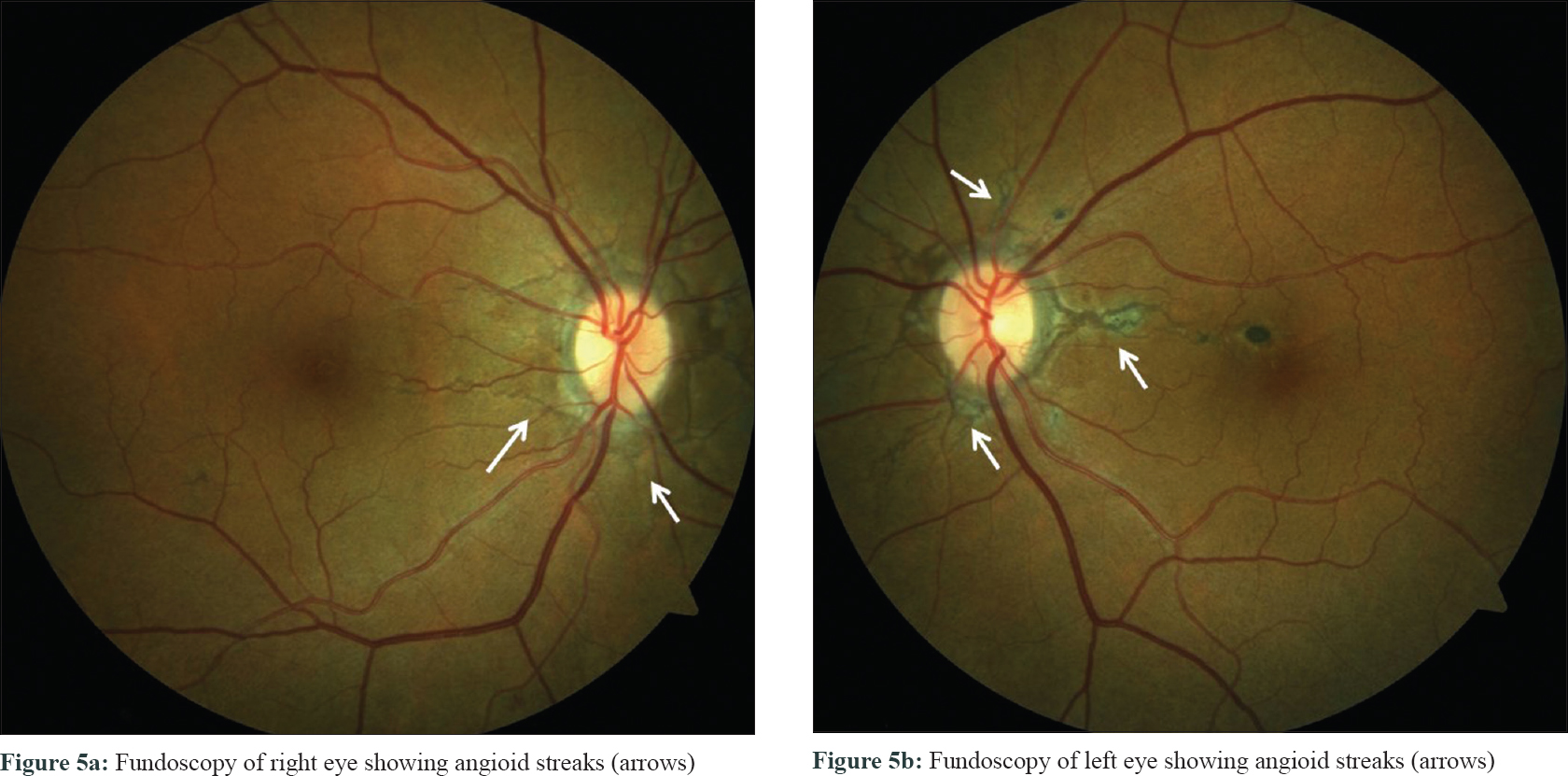 |
| Figure 5 |
Three punch biopsies were performed from the patch and plaque lesions on the abdomen, the axillary and lumbar area of the skin. Histopathologic examination of these three biopsies showed circumscribed nodular foci of ossification with irregularly clumped, basophilic-stained elastic fibers in the mid-dermis [Figure - 6] and [Figure - 7]. Orcein stain revealed thickened, fragmented, curled elastic fibers [Figure - 8] and [Figure - 9] and von Kossa stain demonstrated calcium deposits along the altered elastic fibers [Figure - 10]. The papillary dermis was unaffected. According to these findings, the diagnosis of cutis laxa-like pseudoxanthoma elasticum associated with osteoma cutis was established.
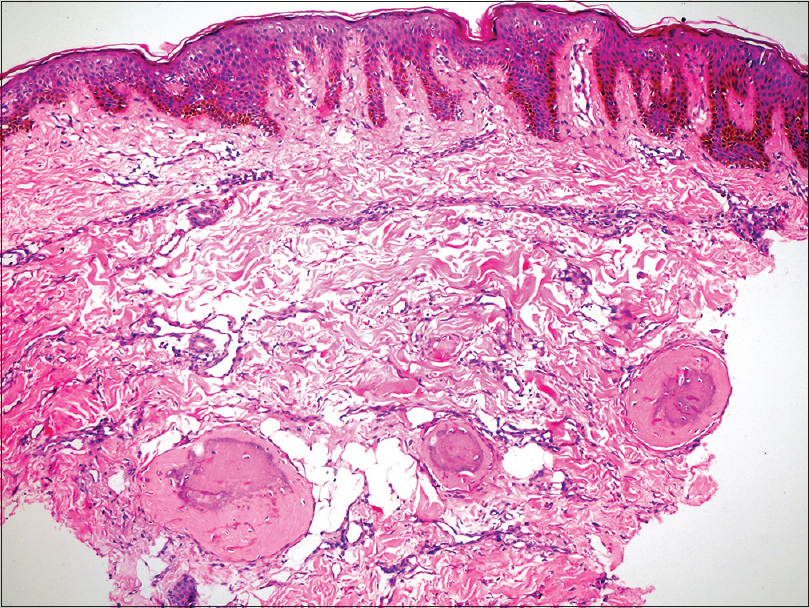 |
| Figure 6: Ossification in the dermis (H and E, ×100) |
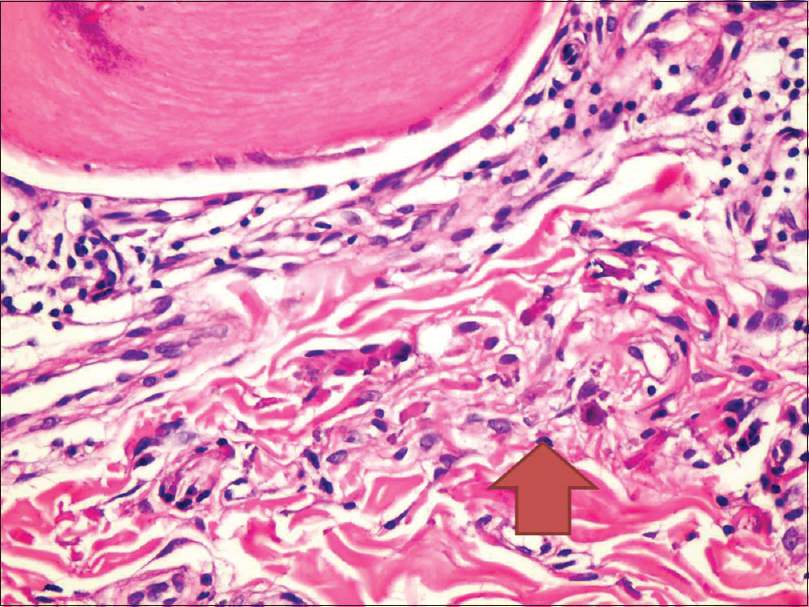 |
| Figure 7: Irregularly clumped, basophilic elastic fibers (red arrow), (H and E, ×400) |
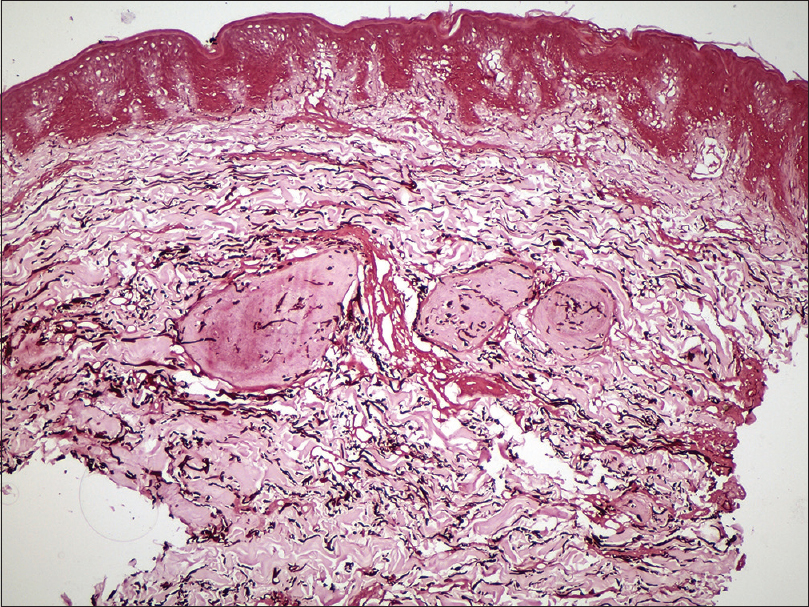 |
| Figure 8: The elastic fibers in the dermis are irregular and haphazard in orientation (Orcein, ×100) |
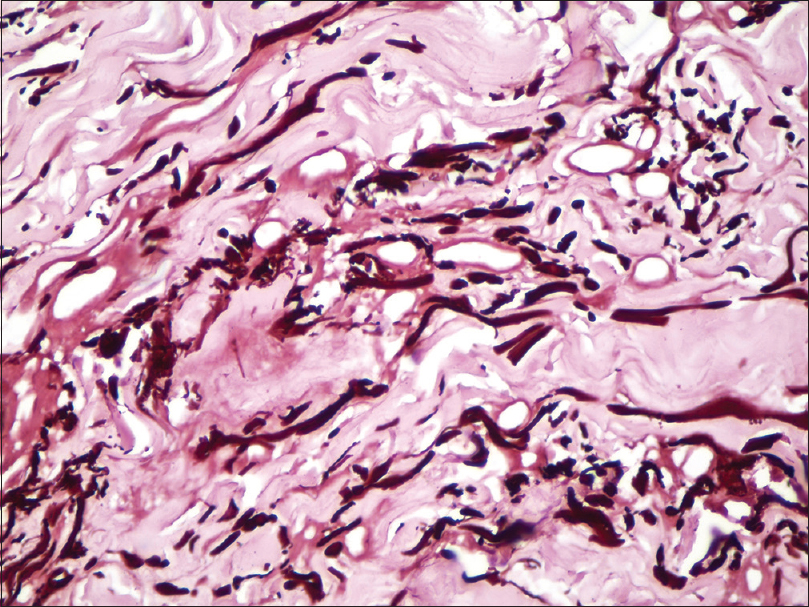 |
| Figure 9: Thickened and fragmented elastic fibers (Orcein, ×400) |
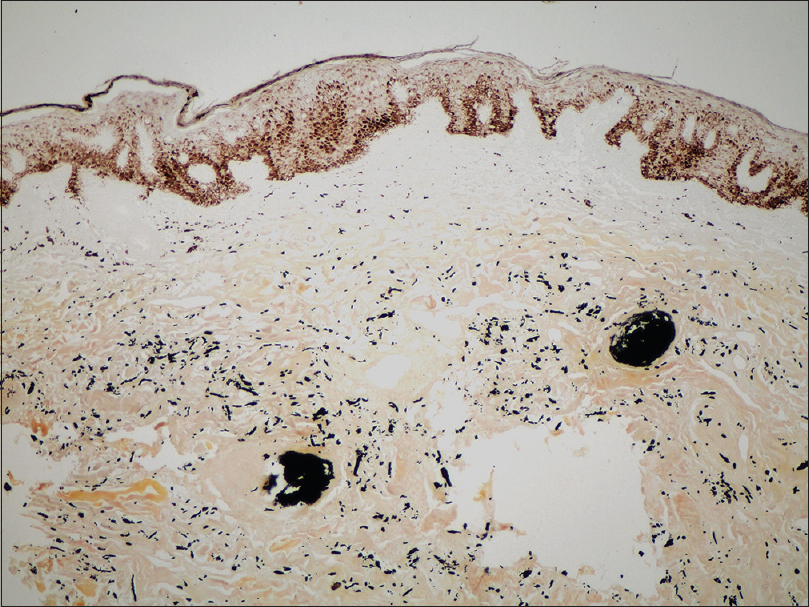 |
| Figure 10: Calcium deposits along the ossification centers and elastic fibers (von Kossa, ×100) |
The presented case was initially diagnosed as cutis laxa because she had excessive loose and wrinkled skin. Nevertheless, histopathologic examination revealed degenerative changes affecting the elastic fibers of the mid dermis and calcium deposits along the elastic fibers characteristic of pseudoxanthoma elasticum. Although degenerated elastic fibers can be seen in cutis laxa, the disease is characterized by a reduction in the number of elastic fibers and calcified elastic fibers are not described.
Another interesting finding in the presented case was ossification. We found only three previous reports of pseudoxanthoma elasticum associated with ossification in literature.[1],[2],[3] On rare occasions, pseudoxanthoma elasticum can mimic reticulate pigmentary disorders.[5] Interestingly, multiple purplish-brown plaques and brown-reticulated patches with ossification were noted in our case. Furthermore, the other cases reported as pseudoxanthoma elasticum with ossification in the literature showed purple plaques,[2] brown-reticulated patches [1] and serpiginous streaks with hyperkeratotic reddish-brown papules.[3]
The development of pseudoxanthoma elasticum is linked to mutations in the ABCC6 gene.[6] The exact mechanism of ABCC6 involvement is unknown. The gene encodes multidrug resistance protein 6, a putative transmembrane adenosine triphosphate-binding cassette transporter protein. Dysfunction of multidrug resistance protein 6 could cause accumulation of compounds with an affinity for calcium.[3] This role of multidrug resistance protein 6 in mineralization suggests the possibility of secondary ossification in pseudoxanthoma elasticum.[3]
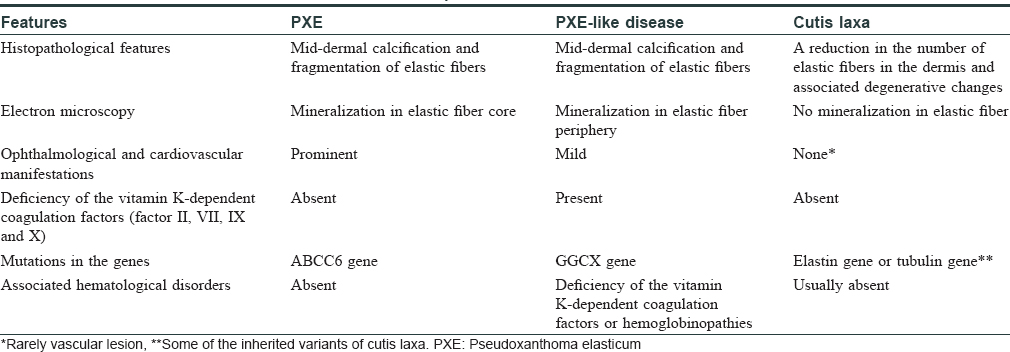
Differentiating pseudoxanthoma elasticum from pseudoxanthoma elasticum-like syndrome and cutis laxa is important [Table - 1]. Pseudoxanthoma elasticum-like syndrome is characterized by a deficiency of the vitamin K-dependent coagulation factors (coagulation factors II, VII, IX, X) or other hematological disorders such as thalassemia, sickle cell anemia and other hemoglobinopathies.[7],[8],[9] Light microscopy will not allow differentiating between pseudoxanthoma elasticum and pseudoxanthoma elasticum-like syndrome.[7],[9] In the presented case, we excluded pseudoxanthoma elasticum-like syndrome owing to fact that no hematological disorders were detected and the laboratory tests such as prothrombin time, activated partial thromboplastin time, factors VII, IX, X were within normal limits.
The characteristic ocular lesion of pseudoxanthoma elasticum is angioid streak, which is a split in Bruch's membrane, an elastin containing membrane behind the retina and observed in our case.[6] Other associated ocular findings include peau d'orange and punched-out peripheral chorioretinal lesions.[10]
We have also found that this was the fourth case of pseudoxanthoma elasticum in the literature which coexisted with osteoma cutis, who had presented with cutis laxa-like cutaneous lesions.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient has given her consent for her images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Choi GS, Kang DS, Chung JJ, Lee MG. Osteoma cutis coexisting with cutis laxa-like pseudoxanthoma elasticum. J Am Acad Dermatol 2000;43(2 Pt 2):337-9.
[Google Scholar]
|
| 2. |
Bahadir S, Cobanoglu U, Siviloglu C, Kapicioglu Z, Baykan M. Cutis laxa-like pseudoxanthoma elasticum with ossification. Int J Dermatol 2004;43:375-8.
[Google Scholar]
|
| 3. |
Lee WJ, Bak H, Chang SE, Lee MW, Choi JH, Moon KC, et al. Autosomal recessive type 2 pseudoxanthoma elasticum presenting with generalized skin laxity. J Dermatol 2009;36:288-92.
[Google Scholar]
|
| 4. |
Schibli H, Stutz SB, Vogel A, Jaeger W, Bersch A, Schnyder UW. Systemic cutis laxa-like pseudoxanthoma elasticum. Hautarzt 1982;33:101-5.
[Google Scholar]
|
| 5. |
Li TH, Tseng CR, Hsiao GH, Chiu HC. An unusual cutaneous manifestation of pseudoxanthoma elasticum mimicking reticulate pigmentary disorders. Br J Dermatol 1996;134:1157-9.
[Google Scholar]
|
| 6. |
Wang WL, Lazar A. Diseases of collagen and elastic tissue. In: Calonje E, Bren T, Lazar AJ, McKee PH, editors. McKee's Pathology of the Skin. 4th ed. China: Elsevier Saunders; 2012. p. 935-66.
[Google Scholar]
|
| 7. |
De Vilder EY, Vanakker OM. From variome to phenome: Pathogenesis, diagnosis and management of ectopic mineralization disorders. World J Clin Cases 2015;3:556-74.
[Google Scholar]
|
| 8. |
Fabbri E, Forni GL, Guerrini G, Borgna-Pignatti C. Pseudoxanthoma-elasticum-like syndrome and thalassemia: An update. Dermatol Online J 2009;15:7.
[Google Scholar]
|
| 9. |
Hosen MJ, Lamoen A, De Paepe A, Vanakker OM. Histopathology of pseudoxanthoma elasticum and related disorders: Histological hallmarks and diagnostic clues. Scientifica (Cairo) 2012;2012:598262.
[Google Scholar]
|
| 10. |
Sapadin AN, Lebwohl MG, Teich SA, Phelps RG, DiCostanzo D, Cohen SR. Periumbilical pseudoxanthoma elasticum associated with chronic renal failure and angioid streaks – Apparent regression with hemodialysis. J Am Acad Dermatol 1998;39(2 Pt 2):338-44.
[Google Scholar]
|
Fulltext Views
4,531
PDF downloads
2,984





![[Figure - 1]](#fig_ijdvl_2017_83_4_464_206721_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2017_83_4_464_206721_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2017_83_4_464_206721_f3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2017_83_4_464_206721_f4.jpg){kind=link}
![[Figure - 5]](#fig_ijdvl_2017_83_4_464_206721_f5.jpg){kind=link}
![[Figure - 6]](#fig_ijdvl_2017_83_4_464_206721_f6.jpg){kind=link}
![[Figure - 7]](#fig_ijdvl_2017_83_4_464_206721_f7.jpg){kind=link}
![[Figure - 8]](#fig_ijdvl_2017_83_4_464_206721_f8.jpg){kind=link}
![[Figure - 9]](#fig_ijdvl_2017_83_4_464_206721_f9.jpg){kind=link}
![[Figure - 10]](#fig_ijdvl_2017_83_4_464_206721_f10.jpg){kind=link}
![[Table - 1]](#tbl_ijdvl_2017_83_4_464_206721_t11.jpg){kind=link}