
Translate this page into:
Demographic and clinicopathological factors associated with biomarker-inflammatory indices and the AMIRI scoring system for predicting acral melanoma mortality-A retrospective study
Corresponding author: Dr. Luiz Fernando Nunes, Department of Bone Connective Tissue Section, Brazilian National Institute of Cancer, Rio de Janeiro, RJ, Brazil. lfernandonunes@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Nunes LF, de Oliveira LC, Barcaui CB, Mendes GQ, Thuler LC, Bergmann A. Demographic and clinicopathological factors associated with biomarker-inflammatory indices and the AMIRI scoring system for predicting acral melanoma mortality-A retrospective study. Indian J Dermatol Venereol Leprol. doi: 10.25259/IJDVL_1198_2024
Abstract
Background
Acral melanoma (AM) is a highly aggressive skin cancer associated with high mortality. In this study, we measured inflammatory biomarkers, identified cutoff values, and developed a scoring system to predict mortality in patients with AM.
Aims
This study aimed to identify inflammatory biomarker cut-off points and factors in AM patients, introducing the Acral Melanoma Inflammatory Risk Index (AMIRI) to predict mortality.
Methods
In this retrospective cohort study, we analysed 394 patients diagnosed with AM. Demographic and clinicopathological data were obtained from medical records. Inflammatory markers (neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), and absolute neutrophil count (ANC)) were measured at diagnosis. The AMIRI scoring system was used to categorise patients into three risk groups: low (AMIRI ≤ 1), intermediate (1 < AMIRI ≤ 2), and high (AMIRI > 2). We used logistic regression models to evaluate associations between inflammatory markers and mortality.
Results
The median age of the 394 AM patients was 67 years. The AMIRI scoring system effectively categorised patients into risk groups, with higher scores correlating with increased mortality risk. The Cox model showed a significant increase in 5-year mortality risk for moderate [OR 1.94] and high [OR 1.96] AMIRI risk groups compared to low-risk patients.
Limitations
This study has limitations, including its retrospective design, being conducted at a single center, incomplete data on adjuvant therapy, and the exclusion of immunotherapy from biomarker analysis, with potential biases from factors like steroid use and associated diseases.
Conclusion
Inflammatory biomarkers are valuable prognostic tools in AM. The AMIRI scoring system effectively stratifies patients, identifying those with higher mortality risk.
Keywords
Absolute neutrophil count
acral melanoma
inflammatory biomarkers
neutrophil-to-lymphocyte ratio
platelet-to-lymphocyte ratio

Introduction
Primary prognostic factors for Acral melanoma (AM) include Breslow’s thickness, ulceration, and sentinel lymph node status.1 As prognostic tools for AM have their limitations, there is an urgent need for the exploration of inflammatory biomarkers to improve understanding. AM generally carries a poorer prognosis than cutaneous melanoma, often due to delays in diagnosis.
Tumour-inflammation interactions are complex, and there is evidence suggesting that inflammation plays a crucial role in tumour initiation, angiogenesis, apoptosis inhibition, and metastasis.2 Alterations in biomarkers such as NLR, PLR, and ANC have been recognised as prognostic indicators for various cancer types.3-8 Despite this, the prevalence and correlation of biomarkers with demographic and clinicopathological variables in AM remain underexplored.
The values of these biomarkers vary across studies due to differences in methodology, population, and study settings. The lack of universally accepted reference values underscores the need for standardised thresholds to improve clinical applicability. Key questions include identifying which values of NLR, PLR, and ANC are associated with higher risk and can effectively distinguish between normal and abnormal results for prognosis and clinical decision-making.
This study aimed to identify cut-off points, prevalence, and factors associated with inflammatory biomarkers in AM patients at a Brazilian Cancer Centre. Additionally, it introduces the Acral Melanoma Inflammatory Risk Index (AMIRI), a novel scoring system designed to predict mortality in AM patients.
Methods
We conducted a retrospective cohort study of patients diagnosed with AM at an Oncology Center in Rio de Janeiro. The study included individuals aged 18 years and older with histopathologically confirmed plantar, subungual, or palmar AM, identified through the pathology database and diagnosed between 2001 and 2015. The study was approved by the Ethics Committee of the Brazilian National Institute of Cancer (CNS Resolution No. 466/12, approval number 3.286.340). Demographic variables collected were age at diagnosis (calculated from the diagnosis date and the patient’s birthdate), gender, and Fitzpatric9 skin type [Table 1]. Clinical-pathological variables comprised melanoma thickness, microscopic ulceration, mitotic rate, and angiolymphatic invasion. Staging at diagnosis (I, II, III, IV) was based on the 2018 AJCC guidelines.10
| Variables | N (%) |
|---|---|
| Age at diagnosis (years) | |
| Median (min-max) | 67.0 (19-96) |
| Sex | |
| Male | 165 (41.9) |
| Female | 229 (58.1) |
| Fitzpatrick skin type | |
| I/II | 208 (52.8) |
| III/IV | 92 (23.4) |
| V/VI | 89 (22.6) |
| Unknown | 5 (1.2) |
| Breslow thickness (mm) | |
| Median | 6.0 |
| Ulceration | |
| No | 74 (18.8) |
| Yes | 282 (71.6) |
| Unknown | 38 (9.6) |
| Mitotic rate | |
| <1/mm2 | 38 (9.6) |
| ≥1/mm2 | 221 (56.1) |
| Unknown | 135 (34.3) |
| Staging (AJCC, 2018) | |
| I | 38 (9.6) |
| II | 221 (56.1) |
| III | 135 (34.3) |
| IV | 0 (0.0) |
| Unknown | 0 (0.0) |
| Lymphovascular invasion | |
| No | 199 (50.5) |
| Yes | 68 (17.3) |
| Unknown | 127 (32.2) |
Min: Minimum observed value, Max: Maximum observed value, AJCC: Melanoma staging according to the American Joint Committee on Cancer (AJCC), 2018 edition.
Inflammatory biomarkers, including NLR (neutrophil-to-lymphocyte ratio), PLR (platelet-to-lymphocyte ratio), and ANC (absolute neutrophil count), were collected from the initial examination report. Time-dependent ROC curves were used to identify optimal cutoff points for predicting 5-year mortality. Sensitivity, specificity, and likelihood ratios were evaluated, with sensitivity measuring true positives and specificity indicating true negatives (longer survival). We prioritised cutoffs with higher specificity to improve prognosis accuracy. Histograms for NLR, PLR, and ANC were also analysed to assess data distribution.
The AMIRI score was based on these biomarkers and assigned points according to defined cutoff values: 1.8 for NLR, 4000 for ANC, and 120 for PLR. Values below and above these cutoff points received 0 and 1 point, respectively. The total score ranges from 0 to 3, where a score of 0 indicates low risk, 1 indicates moderate risk, and 2-3 indicates high risk.
The Kolmogorov-Smirnov test was employed to assess the distribution of variables. Continuous variables are presented as medians, while categorical variables are expressed as percentages. The associations between demographic and clinicopathological factors (age, sex, Breslow thickness, ulceration, mitotic index, and lymphovascular invasion) and inflammatory markers (NLR ≥ 1.8, PLR ≥ 120, and ANC ≥ 4000) were analysed using univariate logistic regression. Odds ratios (OR) with 95% confidence intervals (CI) and p-values were calculated for each variable, with statistical significance set at p < 0.05. Data analysis was performed using SPSS version 23.0.0.
Results
A total of 394 patients with AM were included, with a median age of 67 years (range: 19–96). The majority were female (58.1%) and had Fitzpatrick skin types I/II (52.8%). The median tumour thickness at diagnosis was 6.0 mm, ulceration was present in 71.6% of cases and the mitotic rate was ≥ 1 per mm2 in 56.1% of melanomas. At diagnosis, 9.6% of patients were classified as Stage I, 56.1% as Stage II, 34.3% as Stage III, and 0% as Stage IV [Table 1].
The cut-off points were established as follows: NLR ≥ 1.8, PLR ≥ 120, and ANC ≥ 4,000. Histograms of these biomarkers demonstrated a non-normal distribution [Figure 1]. The area under the curve (AUC) for these biomarkers in ROC analysis was 0.58 (95% CI: 0.52-0.63; p=0.029) for NLR, 0.56 (95% CI: 0.51-0.62; p=0.023) for PLR, and 0.57 (95% CI: 0.52-0.63; p=0.009) for ANC.
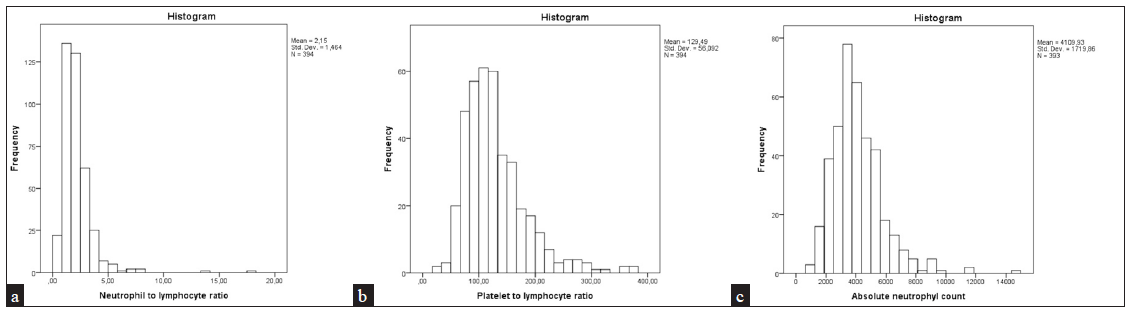
- Histograms representing the distribution of inflammatory biomarkers: (a) Neutrophil-to-lymphocyte ratio (NLR), (b) Platelet-to-lymphocyte ratio (PLR), (c) Absolute neutrophil count (ANC).
NLR showed the highest sensitivity (59.6%) as compared to PLR (54.2%) and ANC (52.7%). Similarly, NLR also showed the highest specificity (48.7%) as compared to PLR (42.9%) and ANC (38.4%). [Figure 2]. An NLR ≥1.8 was observed in 215 patients (54.6%), of whom 122 died (60.1%). A PLR ≥120 was found in 192 patients (48.7%), with 110 deaths (54.2%), while an ANC ≥4,000 was seen in 181 patients (45.9%), resulting in 107 deaths (52.7%) [Table 2].
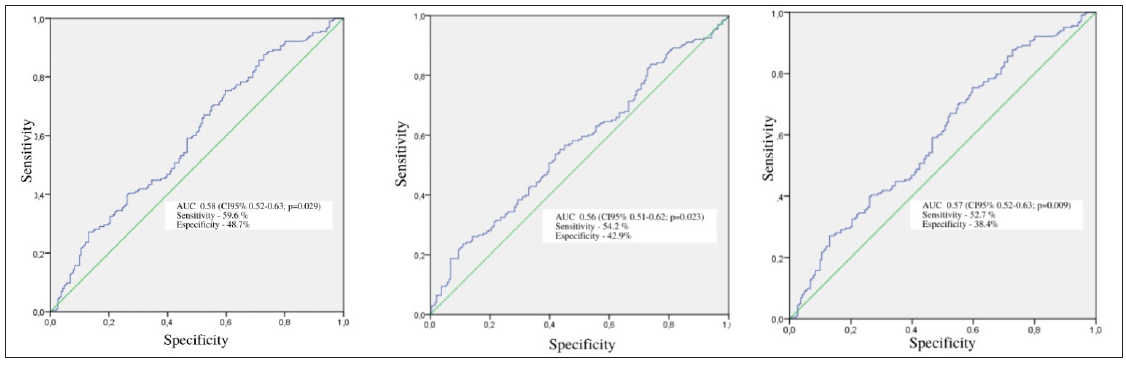
- Analysis of the 5-year OS ROC curve for the NLR, PLR, and ANC in patients diagnosed with AM between 2001 and 2015 (N=394). (The green line represents the “line of no discrimination” (the 45-degree diagonal line). This line indicates a model making random predictions, with no discriminative power between positive and negative classes. The blue line represents the “ROC curve”, which shows the actual performance of the model. The closer this curve is to the top-left corner of the plot, the better the model’s ability to distinguish between classes.)
| N (%) | Death (%) | AUC (CI 95%) | p-value | |
|---|---|---|---|---|
| NLR | ||||
| <1.8 | 179 (45.4) | 81 (39.9) | 0.58 (0.52-0.63) | 0.001 |
| ≥1.8 | 215 (54.6) | 122 (60.1) | ||
| PLR | ||||
| <120 | 202 (51.3) | 93 (45.8) | 0.56 (0.51-0.62) | 0.023 |
| ≥120 | 192 (48.7) | 110 (54.2) | ||
| ANC | ||||
| <4,000 | 213 (54.1) | 96 (47.3) | 0.57 (0.52-0.63) | 0.009 |
| ≥4,000 | 181 (45.9) | 107 (52.7) |
No significant associations were found between demographic and clinicopathological variables with NLR and PLR in univariate analysis. However, ANC ≥ 4,000 was significantly associated with male gender [OR 1.67 (95% CI 1.12–2.50)], ulceration [OR 1.96 (95% CI 1.15–3.35)], and a positive sentinel node [OR 1.86 (95% CI 1.01–3.43)] [see Table 3].
| Variable |
NLR 95% CI (OR 95% CI, p-value) |
PLR 95% CI (OR 95% CI, p-value) |
ANC 95% CI, (OR 95% CI, p-value) |
|---|---|---|---|
| Age at diagnoses | 1.01 (0.99-1.02, 0.378) | 1.00 (0.99-1.02, 0.829) | 0.99 (0.97-1.00, 0.079) |
| Sex | |||
| Female | 1.00 | 1.00 | 1.00 |
| Male | 1.40 (0.93-2.10, 0.103) | 0.98 (0.66-1.47, 0.934) | 1.67 (1.12-2.50, 0.013) |
| Breslow thickness | |||
| T1 | 1.00 | 1.00 | 1.00 |
| T2 | - | 2.00 (0.75-5.33, 0.525) | 0.93 (0.34-2.50, 0.084) |
| T3 | - | 1.04 (0.44-2.47, 0.525) | 0.93 (0.38-2.24, 0.084) |
| T4 | - | 1.29 (0.58-2.84, 0.525) | 1.52 (0.68-3.38, 0.084) |
| Ulceration | |||
| No | 1.00 | 1.00 | 1.00 |
| Yes | 1.31 (0.78-2.19, 0.378) | 1.28 (0.76-2.14, 0.447) | 1.96 (1.15-3.35, 0.033) |
| Mitotic index | |||
| No | 1.00 | 1.00 | 1.00 |
| Yes | 0.61 (0.30-1.24, 0.030) | 0.61 (0.30-1.24, 0.267) | 1.81 (0.88-3.71, 0.267) |
| Lymphovascular invasion | |||
| No | 1.00 | 1.00 | 1.00 |
| Yes | 0.84 (0.48-1.46, 0.826) | 0.72 (0.42-1.25, 0.360) | 1.46 (0.84-2.53, 0.106) |
The AMIRI system categorised patients into risk groups, with higher scores associated with increased mortality [Table 4]. The 5-year overall survival of patients with acral melanoma diagnosed between 2001 and 2015 (N=394) showed significant differences across AMIRI risk categories (Kaplan-Meier, log-rank p<0.001) [Figure 3]. The combination of NLR, PLR, and ANC enhanced prognostication and risk assessment, supporting clinical decision-making.
| Variable | Cutoff value | 0 point (≤ cutoff) | 1 Point (≥ cutoff) |
|---|---|---|---|
| NLR | 1.8 | NLR < 1.8 | NLR ≥ 1.8 |
| ANC | 4,000 | ANC < 4000 | ANC ≥ 4000 |
| PLR | 120 | PLR < 120 | PLR ≥ 120 |
AMIRI score calculation: Total AMIRI score = Points for NLR + Points for ANC + Points for PLR
Risk classification: 0 points: Low risk: 1 point; Moderate risk; 2-3 points: High risk
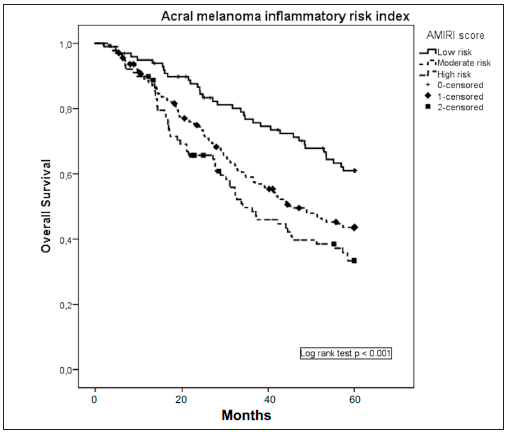
- Overall survival according to acral melanoma inflammatory index (AMIRI), in patients diagnosed with AM, between 2001 and 2015 (N=394).
The Cox model demonstrated a significant increase in 5-year mortality risk for patients with moderate [OR 1.94 (95% CI 1.32–2.85)] and high AMIRI risk [OR 1.96 (95% CI 1.28–3.02)] compared to those with low risk [Table 5]
| Variables | Univariate (HR 95% CI) | p-value | Multivariate (HR CI 95%) | p-value |
|---|---|---|---|---|
| Age at diagnosis (years) | 1.00 (0.99-1.02) | 0.484 | ||
| Sex | 0.032 | |||
| Female | 1.00 | |||
| Male | 1.35(1.03-2.00) | |||
| Breslow thickness (mm) | 1.02(1.01-1.02) | <0.001 | 1.01(1.01-1.02) | 0.021 |
| Ulceration | <0.001 | <0.001 | ||
| No | 1.00 | 1.00 | ||
| Yes | 3.88(2.35-6.39) | 3.08(1.82-5.20) | ||
| Unknown | 1.50(0.73-3.10) | 1.03(0.49-2.20) | ||
| Mitotic rate | <0.001 | |||
| <1 per mm | 1.00 | |||
| ≥1 per mm | 3.76 (1.84-7.70) | |||
| Unknown | 2.95 (1.41-6.14) | |||
| Lymphovascular invasion | 0.002 | 0.003 | ||
| No | 1.00 | 1.00 | ||
| Yes | 1.87(1.31-2.66) | 1.87(1.29-2.71) | ||
| Unknown | 1.07(0.79-1.48) | 1.10(0.76-1.58) | ||
| AMIRI risk | <0.001 | 0.002 | ||
| Low | 1.00 | 1.00 | ||
| Moderate | 1.76(1.21-2.56) | 1.93(1.32-2.85) | ||
| High | 2.31(1.52-3.51) | 1.96 (1.28-3.02) |
Bold values represent variables that remained statistically significant after model adjustments with the table variables: Breslow thickness (p=0.021), ulceration (p<0.001), lymphovascular invasion (p=0.003), and AMIRI risk score (p=0.002).
Discussion
We investigated the prognostic significance of biomarkers and inflammatory indices in AM patients, identifying cutoff points associated with an increased risk of death. No significant associations with clinicopathological variables were found. We also introduce the AMIRI scoring system, a promising tool for improving risk stratification in AM patients.
This study emphasises the role of inflammatory biomarkers in AM, particularly NLR, PLR, and ANC. The identified cutoff values (NLR ≥ 1.8, PLR ≥ 120, ANC ≥ 4,000) provide a basis for risk assessment and prognosis, addressing a gap in existing literature. However, the modest AUC values in the ROC analysis highlight the heterogeneity of AM, suggesting that these biomarkers alone may not serve as definitive prognostic indicators.
Despite modest AUC values, the sensitivity and specificity of NLR, PLR, and ANC offer valuable clinical insights. The high sensitivity of NLR (59.6%) effectively identifies at-risk patients, while PLR’s high specificity (42.9%) helps identify those with a favorable prognosis. These findings highlight the complex role of biomarkers in shaping the multiple factors that affect the course of AM.
The association between elevated biomarkers (NLR ≥ 1.8, PLR ≥ 120, and ANC ≥ 4,000) and higher mortality in the AM cohort underscores their prognostic potential, helping identify patients with more aggressive disease. This insight could be crucial for tailoring treatment and surveillance strategies.
Previous studies have highlighted the prognostic value of inflammatory biomarkers such as neutrophil, lymphocyte, and platelet counts, as well as indices like NLR and PLR, in various cancers.11-15 Accurately predicting prognosis is essential for treatment selection and survival improvement in AM patients. However, our study found that NLR, PLR, and ANC had low accuracy in predicting 5-year survival (AUCs of 0.58, 0.56, and 0.57, respectively) compared to the AJCC TNM staging system.16
While NLR shows promise as a prognostic marker in cancer, no universal cutoff has been established and the literature reports varying results owing to differences in methods and populations.14 This indicates a need for reference values to improve the use of NLR. Our findings suggest that biomarkers and inflammatory indices alone are insufficient for survival predictions or treatment decisions, and further research is needed to identify other potentially useful markers.
The role of systemic inflammation in tumour progression has been well studied but its relationship with demographic and clinicopathological factors remains less explored, particularly in AM.2,15 These associations may differ across tumour types, and no studies have yet explored this in AM. We found no significant associations between NLR, PLR, ANC, and clinical variables suggesting that the tumour microenvironment may influence biomarker levels independently of clinical factors.
Higher death rates observed in our study in patients with inflammatory markers above the cutoff suggest a link between systemic inflammation and tumour burden. This may explain the association between elevated biomarkers and poorer outcomes in advanced stages of AM. Whether this inflammatory response (increased NLR, PLR, and ANC) helps protect against progression remains to be determined.
Previous studies in melanoma patients undergoing immunotherapy have shown that high ANC is associated with worsened overall survival.16 We hypothesize that an elevated baseline ANC (≥4,000), common in lesions without regression, may indicate poor prognosis in AM, though it may not be an independent factor. However, this remains controversial.17
The specific cutoffs for NLR (1.8), PLR (120), and ANC (4,000) in our study differ from those used in the general melanoma population. In a study of 1,351 melanoma patients, poor survival was linked to baseline NLR < 2.5 and PLR < 100.8 Similarly, a study of 742 melanoma patients found that an NLR ≥ 2 was associated with poorer prognosis and reduced survival rates.18
The AUC values for NLR, PLR, and ANC were 0.58, 0.56, and 0.57, respectively, suggesting moderate discriminatory power. However, the prognostic significance of these cutoffs may vary in the broader melanoma population. These biomarkers show unique potential for predicting mortality and clinicopathological features in AM, warranting further analysis.
The AMIRI scoring system enhances mortality prediction in AM patients. The Cox model revealed a significant increase in 5-year mortality for patients in the moderate-risk [OR 1.94 (95% CI 1.32-2.85)] and high-risk [OR 1.96 (95% CI 1.28-3.02)] groups compared to low-risk individuals. These findings remained consistent after adjusting for gender, Breslow thickness, ulceration, angiolymphatic invasion, tumour-infiltrating lymphocytes, and mitotic index. The AMIRI system improves risk stratification, aiding treatment and follow-up. These results support the use of AMIRI for personalised care, though further research with larger cohorts is needed.
Limitations
This study has several limitations. It was conducted at a single center, the National Institute of Cancer in Rio de Janeiro, and its retrospective design may have introduced selection and information bias. Treatment variations across different surgeons and oncologists may have influenced the outcomes. Additionally, data on adjuvant therapy, particularly for stage III and IV patients, were incomplete.
Inflammatory biomarkers can be affected by factors such as steroid use, coronary heart disease, and metabolic syndrome, but documentation of these conditions was limited. Immunotherapy, which is not yet standard care, was not included in the biomarker analysis. However, a strength of the study is its large cohort from a referral center.
Conclusion
The ROC curve analysis identified optimal cut-off values for NLR, PLR, and ANC in AM patients: 1.8, 120, and 4,000, respectively. These biomarkers proved to be valuable prognostic tools. Patients with NLR (p=0.001), PLR (p=0.023), and ANC (p=0.009) values exceeding these cut-offs had higher mortality rates. No significant associations were found between demographic or clinicopathological variables and inflammatory biomarkers.
This study highlights the prognostic value of AMIRI in assessing mortality risk in AM patients. The AMIRI system classifies patients into risk categories, supporting clinical decision-making. Higher risk scores were associated with increased mortality.
In conclusion, this research underscores the importance of biomarker-inflammatory indices in AM prognosis, offering a tool for personalized care and improved outcomes. Further validation in larger cohorts and diverse settings is needed.
Ethical approval
The study was approved by the Ethics Committee of the Brazilian National Institute of Cancer (CNS Resolution No. 466/12, approval number 3.286.340).
Declaration of patient consent
As it is a retrospective study, the signing of the informed consent form was waived.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
References
- Acral melanoma: A retrospective cohort from the Brazilian National Cancer Institute (INCA) Melanoma Res. 2018;28:458-64.
- [CrossRef] [PubMed] [Google Scholar]
- Immunity, inflammation, and cancer. Cell. 2010;140:883-99.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Metastatic renal carcinoma comprehensive prognostic system. Br J Cancer. 2003;88:348-53.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Prognosis and management of thick and ultrathick melanoma. Am J Clin Oncol. 2019;42:824-9.
- [CrossRef] [PubMed] [Google Scholar]
- The prognostic role of platelet-to-lymphocyte ratio on overall survival in gastric cancer: A systematic review and meta-analysis. BMC Gastroenterol. 2020;20:16.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Clinicopathologic analysis of malignant melanoma in Taiwan. J Am Acad Dermatol. 1999;41:945-9.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical significance of preoperative neutrophil-lymphocyte versus platelet-lymphocyte ratio in patients with operable colorectal cancer. Biomarkers. 2012;17:216-22.
- [CrossRef] [PubMed] [Google Scholar]
- Baseline neutrophil-lymphocyte and platelet-lymphocyte ratios as biomarkers of survival in cutaneous melanoma: A multicenter cohort study. Ann Surg Oncol. 2018;25:3341-9.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- “Soleil et peau”[Sun and skin] Journal de Médecine Esthétique. 1975;2:33-4.
- [PubMed] [Google Scholar]
- Melanoma staging: American joint committee on cancer (AJCC) 8th edition and beyond. Ann Surg Oncol. 2018;25:2105-110.
- [CrossRef] [PubMed] [Google Scholar]
- Prognostic role of platelet to lymphocyte ratio in solid tumors: A systematic review and meta-analysis. Cancer Epidemiol Biomarkers Prev. 2014;23:1204-12.
- [CrossRef] [PubMed] [Google Scholar]
- The relationship between the presence and site of cancer, an inflammation-based prognostic score and biochemical parameters. Initial results of the Glasgow Inflammation Outcome Study. Br J Cancer. 2010;103(6):870-6.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Ratio of neutrophil to lymphocyte counts--rapid and simple parameter of systemic inflammation and stress in critically ill. Bratisl Lek Listy. 2001;102:5-14.
- [Google Scholar]
- Prognostic role of neutrophil-to-lymphocyte ratio in breast cancer: A systematic review and meta-analysis. Breast Cancer Res. 2017;19:2.
- [Google Scholar]
- The systemic inflammation-based Glasgow Prognostic Score: A decade of experience in patients with cancer. Cancer Treat Rev. 2013;39:534-40.
- [Google Scholar]
- Baseline biomarkers for outcome of melanoma patients treated with pembrolizumab. Clin Cancer Res. 2016;22:5487-96.
- [Google Scholar]
- Overall survival with combined nivolumab and ipilimumab in advanced melanoma. N Engl J Med. 2017;377:1345-56.
- [Google Scholar]
- Basal neutrophil-to-lymphocyte ratio is associated with overall survival in melanoma. Melanoma Res. 2017;27:140-4.
- [Google Scholar]




