Translate this page into:
Dermatology nursing in India: The journey thus far
Correspondence Address:
Vineet Kaur
International Skincare Nursing Group, Brij Enclave, Sunderpur, Varanasi
India
| How to cite this article: Kaur V. Dermatology nursing in India: The journey thus far. Indian J Dermatol Venereol Leprol 2012;78:527-531 |
The increasing burden of skin disease has put an enormous strain on the already fragile health system of India. Various studies from India have shown that the majority of attendances in primary care clinics [1],[2] are for dermatological consultations. A study from northern India [3] has demonstrated that, at any given time, about one third of school children suffer from some skin condition. A similar situation exists in parts of the developed world too. [4] Although a primary health care system is in place to cater to the health needs of rural India, it barely copes with the demands of patients with skin diseases because of the very little teaching of dermatology during the undergraduate program for doctors. Surprisingly, this is a global phenomenon. The "Models of Integrated Service delivery in Dermatology" report by the Dermatology Workforce Group, UK 2007 [5] states that "Disappointingly, education in dermatology at all levels and for all professionals is very limited." Also, the importance of a speciality is directly linked, unfortunate though it is, with the number of emergencies associated with it. By this yardstick, it is easy to see why dermatology has not received its due priority. Sadly, what is often missed is the ′burden′ of skin disease in terms of psychosocial and financial consequences. Quality of life issues are mostly not accounted for in most studies from the subcontinent.
Add to this scenario the fact that most dermatologists are based in urban areas. Often, a dermatologist is "out of reach" for the majority of patients in rural India. The transport system in most of these parts is sketchy. Therefore, in effect, only very meager specialist dermatologic services are available at the periphery.
The scene in the towns and cities, where most dermatologists are based, too is not very encouraging. Whether it is in a hospital or in a private clinic, the doctor patient ratio is often very low and the consultation time in these situations is very brief. In such situations, it would be unreal to expect a full and detailed explanation of the patient′s condition, prognosis, and details regarding the often elaborate treatments prescribed, leave alone any information on prevention. In government hospitals, the numbers of nurses posted in a department are related to the number of beds, irrespective of the load in the OPD. It is a general observation that nurses are seldom posted in Skin OPDs, [6] and even if they are, they mostly play administrative or housekeeping roles.
Nursing, on the other hand, is primarily a patient-centric activity. Traditionally, nurses, from the time of Florence Nightingale, have anointed the sick, held their hands, given them a patient hearing - in fact been involved in all activities that have one thing in common - time spent with the patient. Therefore, while the dermatologist tries to handle large numbers, a nurse could balance the act with her educational role, support, touch, and time.
Some years ago, the situation was similar in what we call today the ′developed world.′ They responded to this need by harnessing the vast resource of nurses who were then trained in basic skin care. With increasing collaboration with their dermatology colleagues, some of them trained further in dermatology to assume leadership roles as specialist dermatology nurses. One of the pioneers in the field was the Oxford Department of Dermatology. Here, the role of the dermatology liaison nurse was developed for the first time, and it was evidenced that nurse input could greatly impact the quality of self-management of chronic skin conditions as well as result in averting many hospital readmissions. [7] This model was subsequently replicated in many parts of UK. Other studies from around the world too showed the difference, nurses as part of dermatology teams, had made in both dependent and independent roles (nurse - led clinics). [8],[9],[10],[11] These studies have also highlighted the fact that patients with chronic skin diseases do best when a trained nurse is involved in their care.
This exposure to the concept of ′dermatology nursing′ sowed the seeds for the idea of introduction of a similar concept back home in India. In the year 2003, after being appointed to the advisory board of the International Skincare Nursing Group (ISNG) as the only dermatologist, the author in her interaction with pioneering nurses from across the globe, received great insight. It became evident that the nurses had great potential and that they could make a significant difference to patient care, given the right knowledge and support.
The curriculum of pre-registration nurses was examined and it showed great variation between states. For example, in Uttar Pradesh, average of 10 lectures during the three years degree course were mandatory. There was some teaching of hygiene in the first year, but dermatology per se was covered under the topics of allergies, congenital anomalies, eczemas, infections, psoriasis, pemphigus, and tumors only in the II nd year and that too with no direct teaching of nursing interventions in these conditions. In the III rd year, leprosy was discussed under community health training.
Then, in 2004, at the national conference of the IADVL (Dermafest 2004), the first focus session on dermatology nursing was held. The session was well attended, especially by the local nurses and nursing tutors. Speakers from India and the United Kingdom shared their experiences and views on the scope of this specialty of nursing in India. The process of sensitization towards the valuable role of nurses had begun.
A study was conducted [6] around this time to ascertain the existing level of knowledge of nurses posted in dermatology wards in tertiary level hospitals around the country. Twenty-seven centers in the country participated. These nurses had been posted for periods ranging from a few months to up to 5 years. Analysis of the data revealed that they were mostly involved in activities like making beds, dispensing medication, and stock keeping. There was no direct skin care role, which clearly reflected in their knowledge of the common issues of skincare like cleansing. Knowledge of even the common skin conditions, for which patients were admitted to their wards, was negligible.
In the larger picture, as with any new concept, there were supporters and detractors. In the ensuing year, these mixed feedbacks continued. While dermatology nursing globally was standing on firmer feet by the day, the journey in India had only just begun. Some dermatologist colleagues had by now begun some informal teaching (mostly on ward rounds) for nurses posted in their wards.
Besides nurses posted in wards, it became increasingly important to address the learning needs of nurses in the field and community. A project to train Auxiliary Nurse Midwives in skin care in a rural health center run by Christian missionaries was conducted. [12] Twenty-five ANMs working in a government primary health center were recruited on a first-come basis to undergo a 6 month training program (2 sessions per month) in skin care. Diagnosis and management of 10 common skin diseases were taught using flash cards and clinical photographs supplemented by clinical cases brought in by the ANMs themselves from their communities. Importance of skin hygiene and the use of indigenously available medicines were emphasized. An ongoing assessment of their acquired skills was made from their approach to diagnosis and management of cases. Their level of interest was assessed based on their attendance and their efforts to bring cases from their communities for discussion, whereas pre- and post-testing questionnaires were used to evaluate their knowledge acquired. This assessment was made using a three-grade scale for each ANM. The long-term usefulness was assessed on the basis of records of patients seen, diagnosed, managed, and referred by each trained ANM.
The next Dermacon 2005 in New Delhi saw continued deliberations on the subject of how we needed to harness the skills of nurses to improve patient care. Prof Terence Ryan, one of the pioneers in establishing dermatology nursing roles in the UK, was a key speaker. There were demonstrations on wet wraps by a nurse member of ISNG, and the role of the dermatology nurse in day care was discussed in detail.
The Annual national conference of IADVL in Hyderabad (Dermacon 2006) saw a further thrust with the Chair of ISNG and Professor of Nursing, Dr Steven Ersser, lending his support to the Indian efforts by participating in the focus session. He spoke on ′nursing interventions for dry skin,′ while Prof Ryan talked about the integrated approach to skin and wound care. Dr. Kaur addressed the crucial role that nursing of the skin in dermatological emergencies played. With this wide new perspective on the various reasons, why nurses can prove valuable players in the delivery of optimal skincare, the support for the concept grew. Prof Ersser applauded the Indian efforts greatly. [13]
The ball had been set rolling and continued to gain momentum. At Chennai, the following year (Dermacon 2007), the author presented results from a study [14] that showed the difference in treatment outcome with the intervention of a trained nursing assistant in the OPD in patients of acne. Forty patients with grade II acne vulgaris were included in the study. Patients were randomly divided into 2 groups - Group A saw only the dermatologist, and Group B were counseled by a trained dermatology assistant following the dermatologist consultation. The results show that the percentage of patients showing no improvement was greater in Group A. (17.6%) as compared to group B (5.0%). Also, a larger percentage of patients in group B reported good and satisfactory improvement. It can, therefore, be deduced that where there was additional nursing intervention, the outcome was better. This was one of the first studies conducted to show the impact of nursing intervention in India.
The same year, at the 21 st World Congress of Dermatology (WCD) in Buenos Aires, the author was invited to talk about the ′Developments in dermatology nursing care in India.′ This was one of the first international events where India had arrived on the world map of dermatology nursing. There was resounding appreciation of the efforts made in India and led to many opportunities for networking with others in the field. It also brought to the front that across the world, there has been great resistance to the inclusion of nurses in dermatology teams.
The 36 th Annual conference of the Indian Association of Dermatologists, Venereologists, and Leprologists (Dermacon 2008), held at Chandigarh, also had a focus session on dermatology nursing. The need to carry out training of general nurses posted in dermatology departments by consultants was emphasized. A unifying theme for all parts of the country in terms of teaching basic skincare with low technology to all nurses at all levels was discussed.
Increasingly more began to be written about dermatology nursing in its various roles in standard text books [15] and journals. [16] Internationally, India began to be mentioned amongst the few countries that were seen to launch this concept in their skin care delivery system. [17]
The growing support for dermatology nursing culminated in the establishment of a Special Interest Group (SIG) on dermatology nursing by the Indian Association of Dermatologists, Venereologists, and Leprologists (IADVL) as part of the IADVL Academy in July 2010. The team presently includes:
International advisers: Prof. Steven Ersser (UK)
Mrs. Barbara Page (Scotland)
Prof. Anil K Jha (Nepal)
Task Force members: Prof. SS Pandey (Varanasi)
Prof. Y Marfatia (Vadodara)
Prof. AK Khare (Udaipur)
Prof. Uday Khopkar (Mumbai)
Lt. Col. P Vijendran (Armed Forces)
Dr. Iffat Hassan (Srinagar)
National Coordinator: Dr. Vineet Kaur (Varanasi)
The aims and objectives of the SIG are as follows:
- Study of the present knowledge, attitude, and practice of skin care in skin disease, leprosy, and STDs including HIV/AIDS among nurses posted in dermatology and STD units in their respective states using uniform questionnaires (prepared by the task force members).
- Organizing workshops in various medical colleges across the country to address nursing tutors so that dermatology can be better represented in the pre-registration training for all nurses
- Preparing a national curriculum for skin care training for nurses
- Conducting workshops in departments of dermatology to train nurses working in these departments in basic skin care.
- Organizing 6 monthly meetings of the task force to evaluate achievements and to plan further line of action. One meeting would be held on the side lines of the annual national conference.
- Engaging with the Nursing Council of India to influence change of existing curriculum of dermatology for pre-registration nurses
Meanwhile, a curriculum framework [18] for teaching skin care to nurses was prepared and this document was released at the national conference, Dermacon 2011 in Gurgaon. It aims to serve as a road map for what skin care/dermatology to teach pre-registration and general nurses. It has been well-accepted by colleagues across the country.
Around this time, members of the task force conducted a multicentric study of the ′Existing knowledge of dermatology/skincare in nurses working in dermatology units.′ This survey was done using an anonymous questionnaire having 30 questions, which was filled in by the staff nurses in the participating centers. There were a total of 54 respondents from 5 states, including those from the armed forces. The respondents were kept anonymous to avoid the risk of nurses feeling intimidated by this exercise and, therefore, not attempting the questionnaire in all fairness. The survey was conducted with the sole aim of gathering information on their existing level of knowledge, which would then be used as a starting point for further teaching. The results of this study were presented. It highlighted the significant gap in knowledge of nurses already working in dermatology units, some for over 5 years. There were some other very significant findings from the above-mentioned study. The fact that language is a major barrier came forth. A large percentage of the questions were not understood by nurses, especially from Rajasthan and Uttar Pradesh, perhaps because some of the teaching is carried out in Hindi or regional languages. This is important because the Nursing Council of India recommends all textbooks for nurses in English, which might be only partially understood in the various states. As previously known, most nurses seemed to be carrying out only general medical duties like bed-making and dispensing medication. Apart from the nurses of the armed forces, there appeared to be no direct involvement of these nurses in the care of the patients admitted in the skin wards.
At the 22 nd World Congress of Dermatology, Seoul 2011, the achievements of the IADVL through the establishment of a SIG for dermatology Nursing were presented.
Since one of the thrust areas of the SIG is to take knowledge of skincare to every nurse, a one-day workshop was conducted in the College of Nursing, Banaras Hindu University, Varanasi, on 31 st July 2011. Wide ranges of topics were addressed ranging from the anatomy and physiology of the skin to various common skin conditions and dermatological therapy. There were 54 participants from the II nd year degree course. A pre- and post-test was carried out through questionnaires, which consisted of 30 questions. The highlight of the workshop was the interactive session where student nurses were handed out dummy prescriptions of common skin conditions and were asked to discuss how they would deal with such patients and explain therapy in individual cases. Analysis of the pre- and post-test questionnaires showed an overall 28.1% improvement in the knowledge of the participants.
Encouraged by the success of this workshop, the first zonal level workshop on basic skincare was organized at Mangalore on 7 th and 8 th January 2012. The two-day workshop covered the entire range of common skin conditions along with pharmacology and psychological aspects of skin disease. The 271 participants who attended the workshop (included nursing students from different years of the BSc, MSc, and PhD programs as well as nursing tutors), were exposed, mostly for the first time, to their great potential as caretakers of the skin. The interactive sessions on both days saw their active participation in discussing case studies with the objective of highlighting their role as members of the dermatology team. Results from an immediate pre- and post-test questionnaire study showed an overall improvement of 29.23%.
In the changing and ever-improving scenario of provision of health care, nurses should no longer be seen executing their traditional roles only. They are a resource worth tapping for the larger good of the patient community. They have specific roles to play in skin care across the entire spectrum of skin diseases - both acute (dermatologic emergencies) and chronic. With specialized training, they can make effective counselors for patients and care givers alike, in chronic relapsing skin conditions like psoriasis and atopic dermatitis.
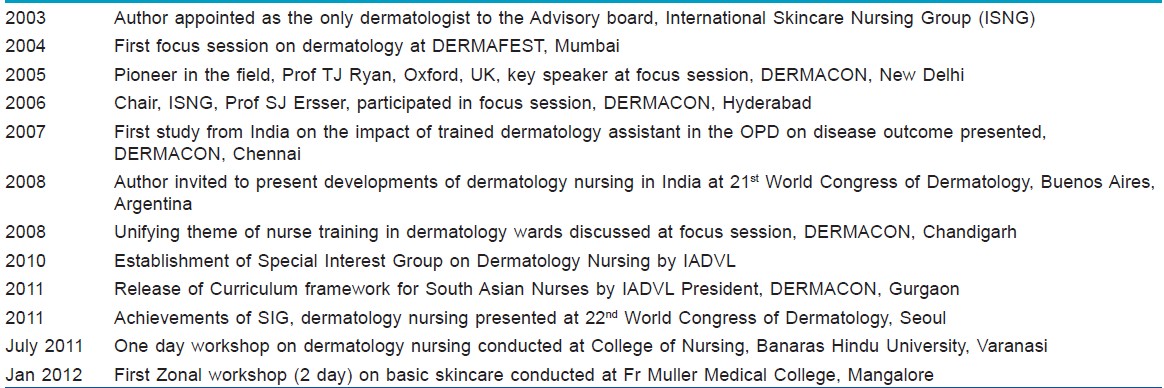
Dermatology nursing in India has travelled this far over the last 8 years [Table - 1], and there are many more miles to cover. Although the journey has been challenging, with the growing acceptability of the concept and support of colleagues, there is definitely bright light at the end. The future demands that in order to achieve our goals, the dermatology fraternity must work alongside colleagues in colleges of nursing and the Indian Nursing Council to raise the profile of dermatology nursing. The curriculum must be reinvented to address more common and relevant issues in skin health and disease so that it appeals to student nurses. Hospital administrators should be convinced of the great need for nurses in skin outpatient departments.
| 1. |
Kaur P, Singh G. Community dermatology in India. Int J Dermatol 1995;34:322.
[Google Scholar]
|
| 2. |
Grover S, Ranyal RK, Bedi MK. A cross section of skin diseases in rural Allahabad. Indian J Dermatol 2008;53:179-81.
[Google Scholar]
|
| 3. |
Dogra S, Kumar B. Epidemiology of skin diseases in school children: A study from northern India. Pediatr Dermatol 2003;20:470-3.
[Google Scholar]
|
| 4. |
Lowell BA, Froelich CW, Federman DG, Kirsner RS. Dermatology in primary care: Prevalence and patient disposition. J Am Acad Dermatol 2001;45:250-5.
[Google Scholar]
|
| 5. |
Dermatology Workforce Group. Models of Integrated service delivery in Dermatology. London: All Party Parliamentary Group; 2007.
[Google Scholar]
|
| 6. |
Kaur V. Developments in dermatology nursing in India. Lecture delivered at the 21 st World Congress of Dermatology, Buenos Aires, Argentina; 2007.
[Google Scholar]
|
| 7. |
Steven JE, Newton JN, Taylor HR, Van Onselen J, Kaur V. A descriptive and evaluative study of a Dermatology Nursing Service. NHS R&D document (Report no.5). Oxford: OCHRAD; 1998.
[Google Scholar]
|
| 8. |
McKee M, Nolte E. Responding to the challenge of chronic diseases: Ideas from Europe. Clin Med 2004;4:336-42.
[Google Scholar]
|
| 9. |
Cork MJ, Britton J, Butler L, Young S, Murphy R, Koehane SG. Comparison of parent knowledge, therapy utilization and severity of atopic eczema before and after explanation and demonstration of topical therapies by a specialist dermatology nurse. Br J Dermatol 2003;149:582-9.
[Google Scholar]
|
| 10. |
Coutenay M, Carey N. Nurse-led care in dermatology: A review of literature. Br J Dermatol 2006;154:1-6.
[Google Scholar]
|
| 11. |
Moore E, Williams A, Manias E, Varigos G. Nurse led clinics reduce severity of childhood atopic eczema: A review of literature. Br J Dermatol 2006;155:1242-8.
[Google Scholar]
|
| 12. |
Kaur V. Dermatology service through Auxiliary Nurse Midwives: An Indian model. Dermatol Nurs 2003;2:18-9.
[Google Scholar]
|
| 13. |
Ersser S. Growing recognition of Dermatology Nursing in India. Dermatol Nurs 2006;5:15.
[Google Scholar]
|
| 14. |
Kaur V. Nursing interventions in dermatology. Presented at 35 th National conference of Indian Association of Dermatologists, Venereologists and Leprologists, Chennai, India; 2007.
[Google Scholar]
|
| 15. |
Kaur V, Singh G. Nursing care for leprosy patients In: Kar HK, Kumar B, editors. IAL Textbook of Leprosy. 1 st ed. New Delhi: Jaypee Brothers Medical Publishers; 2010. p. 468-82.
[Google Scholar]
|
| 16. |
Rajkumar E, Julios S, Salome A, Jennifer G, John AS, Kannan L, et al. Effects of environment and education on knowledge and attitude of nursing students towards leprosy. Indian J Lepr 2011;83:37-43.
[Google Scholar]
|
| 17. |
Ersser SJ, Kaur V, Kelly P, Langoen A, Maguire SA, Nicol NH, et al. The contribution of the nursing service worldwide and its capacity to benefit within the dermatology field. Int J Dermatol 2011;50:582-9.
[Google Scholar]
|
| 18. |
Kaur V. Skincare Nursing for South Asian Nurses - A framework curriculum. 1 st ed. Varanasi: Jauhari Printers; 2010.
[Google Scholar]
|
Fulltext Views
2,842
PDF downloads
1,222





![[Table - 1]](#tbl_ijdvl_2012_78_5_527_100514_b1.jpg){kind=link}