Translate this page into:
Dermatomyositis revealing both a metastatic linitis plastica and hepatitis C virus infection
Correspondence Address:
Imane Alouani
Department of Dermatology, Mohammed VI University Hospital of Oujda, Oujda
Morocco
| How to cite this article: Alouani I, Fihmi N, Zizi N, Dikhaye S. Dermatomyositis revealing both a metastatic linitis plastica and hepatitis C virus infection. Indian J Dermatol Venereol Leprol 2017;83:606-609 |
Sir,
Dermatomyositis is a rare disease, characterized by an inflammatory myopathy and typical cutaneous lesions. Its relationship with cancer is well known.[1] However, its association with hepatitis C virus has rarely been reported in the literature.[2] We report a patient with dermatomyositis revealing a metastatic linitis plastica and hepatitis C virus infection.
An 80-year-old woman with no preceding history of autoimmune disease, malignancy or jaundice was admitted for a periorbital heliotrope rash [Figure - 1] with muscle weakness. She reported having dysphagia with episodes of accidental liquid aspiration, including saliva. Physical examination revealed discrete erythematous papules overlying the interphalangeal joints (Gottron's papules) [Figure - 2] and prominent periungual erythema with ragged cuticles (manicure sign) [Figure - 3]. Manual muscle testing showed proximal muscle weakness (2/5 according to Medical Research Council Scale). Elevated serum muscle enzymes were observed with increased creatine kinase to 426 U/L (normal <170 U/L); the aspartate aminotransferase and lactic dehydrogenase levels were 87 and 546 U/L, respectively (normal aspartate aminotransferase <35 U/L and lactic dehydrogenase 190–400 U/L). Antinuclear antibody, anti-aminoacyl transfer ribonucleic acid synthetase, anti-signal recognition particle, anti-Mi-2 antibody and anti-PM/SCL antibody were all negative. The electromyography revealed proximal muscle-predominant myogenic change with fibrillation waves and abnormal low amplitude and short duration of motor unit action potential. The muscle biopsy showed perifascicular muscle atrophy associated with interstitial fibrosis and perivascular inflammatory cell collections [Figure - 4], [Figure - 5], [Figure - 6]. Based on these findings and on Bohan and Peter's criteria (the five criteria are: symmetric proximal muscle weakness, elevation of serum skeletal muscle enzymes, the electromyographic triad, muscle biopsy abnormalities and typical skin rash of dermatomyositis), a diagnosis of dermatomyositis was made. The patient was started on prednisolone 2mg/kg/day, with improvement in her weakness and dysphagia. Intravenous immunoglobulin therapy was considered, but could not be administered due to financial constraints. Laboratory workup revealed positive hepatitis C antibody with a high titer: 815,000 IU/ml.
 |
| Figure 1: Periorbital heliotrope rash |
 |
| Figure 2: Gottron's papules on the left foot. Note the characteristic erythematous papules overlying the interphalangeal joints |
 |
| Figure 3: Prominent periungual erythema with ragged and painful cuticles on the right hand suggestive of manicure sign |
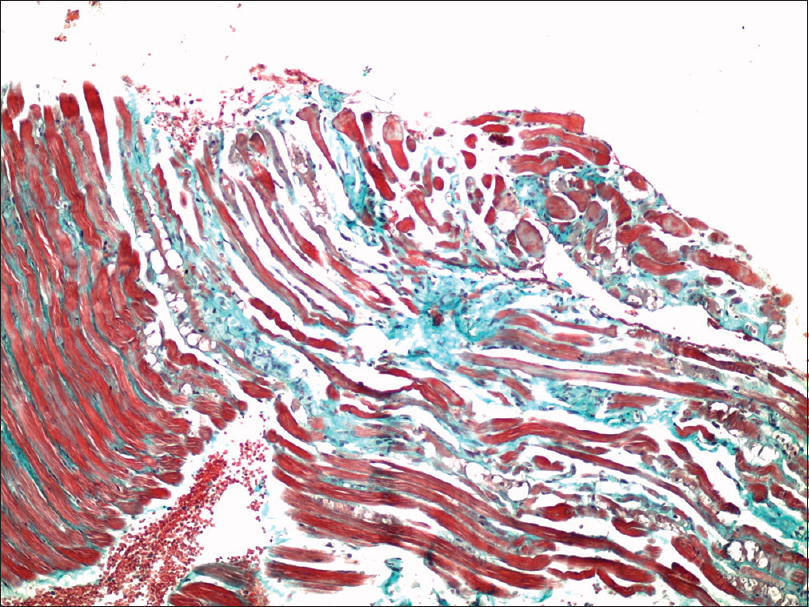 |
| Figure 4: Muscle biopsy showing perifascicular muscle atrophy (Masson's Trichrome, ×100) |
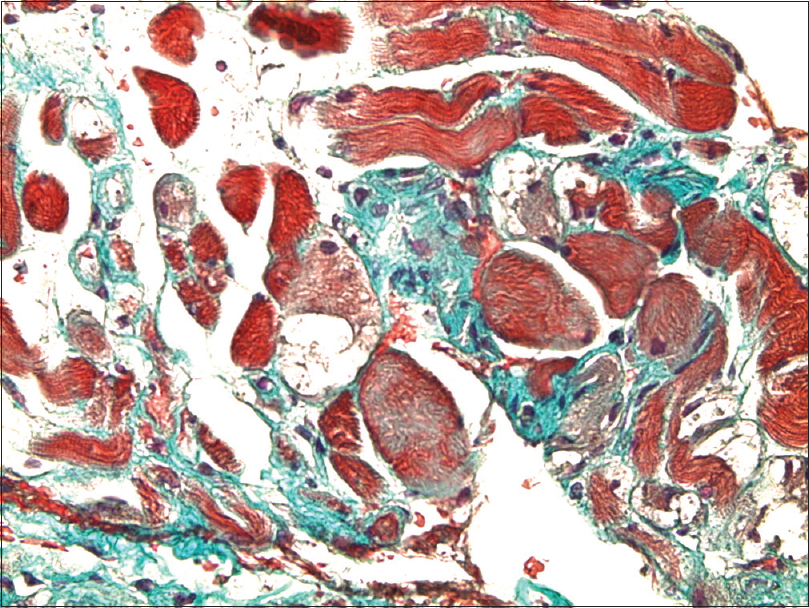 |
| Figure 5: Muscle biopsy showing interstitial fibrosis (Masson's Trichrome, ×200) |
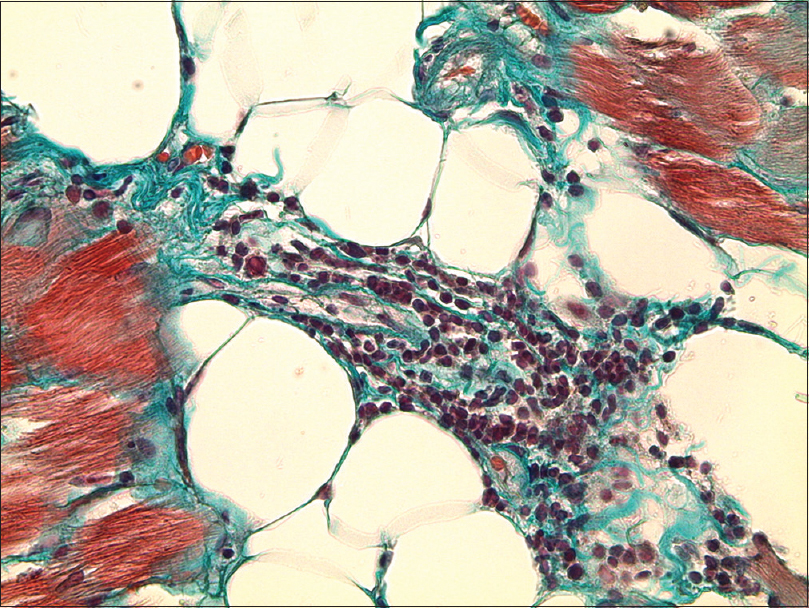 |
| Figure 6: Muscle biopsy showing perivascular inflammatory cell infiltrate (Masson's Trichrome, ×400) |
Cancer screening using thoracic, abdominal and pelvic computed tomography revealed metastatic lesions within the spine and the liver, ascites and peritoneal nodules [Figure - 7]. Digestive endoscopy showed a macroscopically normal gastric mucosa. However, there was a malignant glandular proliferation of independent cells (signet ring cells) in the fibrous stroma histologically [Figure - 8] and [Figure - 9]. Due to the poor prognosis of her metastatic carcinoma (stage T4bN3M1), interferon-based therapy for her hepatitis C could not be started.
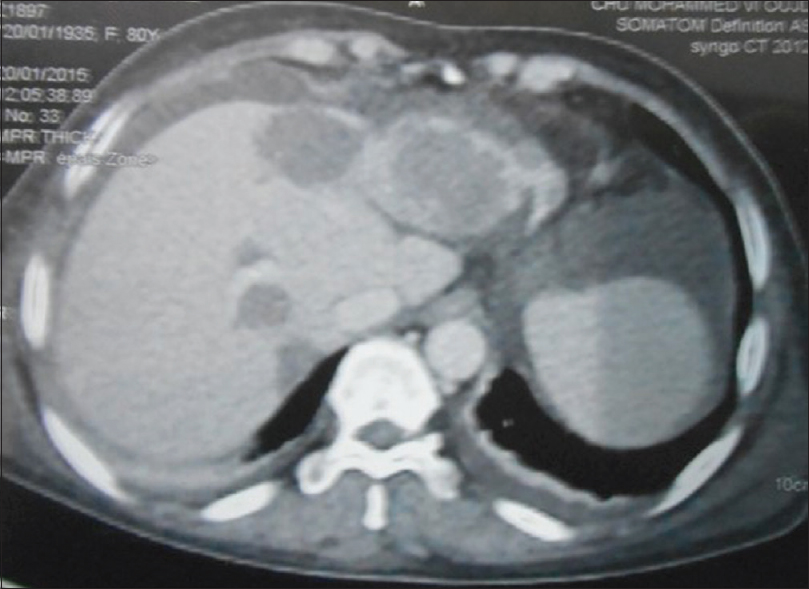 |
| Figure 7: Abdominal computed tomography scan showing hypoattenuating lesions suggestive of liver metastases (arrows) |
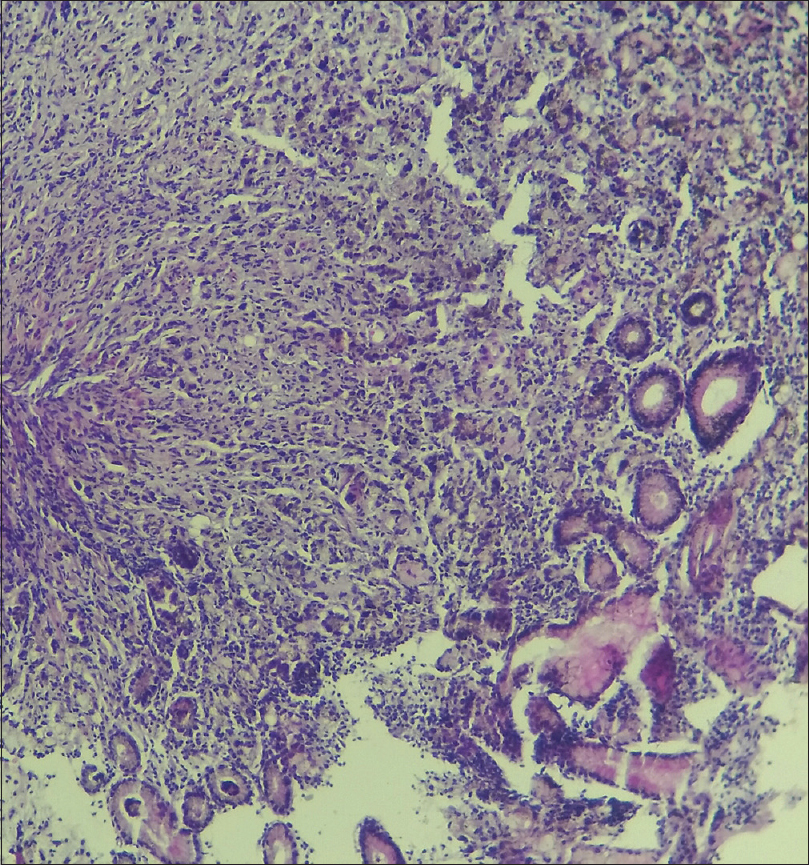 |
| Figure 8: Gastric mucosa biopsy showing tumor proliferation in gastric mucosa (HES, ×10) |
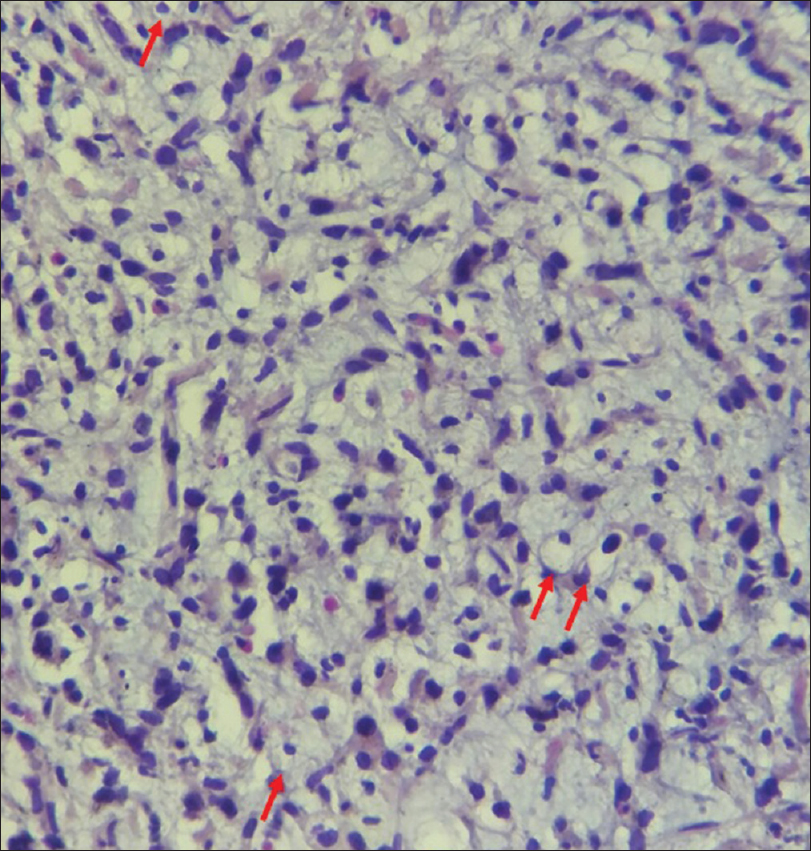 |
| Figure 9: Gastric mucosa biopsy showing signet ring cells (arrows) (HES, ×50) |
Chronic hepatitis C virus infection has been known to be associated with the presence of autoantibodies and various types of autoimmune diseases, leading to the hypothesis that chronic hepatitis C virus infection could cause dermatomyositis through an autoimmune mechanism.[3] However, this coexistence could be coincidental. Studies have been published on the outcome of corticosteroid therapy in patients with chronic hepatitis C virus infection. Some studies have described a rapid progression of the liver disease in immunosuppressed patients with chronic hepatitis C virus infection.[4] In our case, steroids could not be stopped because of the life-threatening consequences of her severe dermatomyositis. During the initial two months of follow-up, the patient did not show any sign of reactivation of her hepatitis. Liver enzymes' status was normal. The patient was then lost to follow-up. The alternative treatment considered was intravenous immunoglobulin therapy. It can be tried in patients with contraindication for corticosteroids.[5] Furthermore, intravenous immunoglobulin has been shown to be effective in most dermatomyositis patients with esophageal involvement.[5]
On the other hand, the relationship between cancer and dermatomyositis has been widely reported in the literature. Recent studies demonstrated that 15%–32% of patients with dermatomyositis are associated with various internal malignancies.[1] Ovarian and breast cancers are the most frequent neoplasms in women.[1] Linitis plastica is a rare, malignant gastric adenocarcinoma characterized by glandular proliferation of signet ring cells in the fibrous stroma.[6] Due to its metastatic stage in the present case, curative surgery could not be proposed. The patient refused the palliative chemotherapy. Terada described in 2013 a patient with dermatomyositis associated with a signet ring cell carcinoma of esophagus.[7] However, after a literature review, no previous association has been noted between dermatomyositis and gastric signet ring cell carcinoma.
This is a rare case of a patient with dermatomyositis, revealing both a metastatic linitis plastica and hepatitis C virus infection. This case emphasizes again the need for tumor screening, when dermatomyositis is diagnosed in advanced adulthood. It raises a discussion about the risk–benefit profile of corticosteroid therapy in the presence of chronic infection, particularly in life-threatening situations such as a severe dermatomyositis.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given her consent for her images and other clinical information to be reported in the journal. The patient understands that name and initials will not be published and due efforts will be made to conceal identity, but anonymity cannot be guaranteed.
Acknowledgment
The authors wish to thank Dr. Mouna Rimani, Dr. Amal Bennani and Dr. Nawal Harchichi, for their valuable assistance to the histopathology photographs.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Hill CL, Zhang Y, Sigurgeirsson B, Pukkala E, Mellemkjaer L, Airio A, et al. Frequency of specific cancer types in dermatomyositis and polymyositis: A population-based study. Lancet 2001;357:96-100.
[Google Scholar]
|
| 2. |
Kee KM, Wang JH, Lee CM, Changchien CS, Eng HL. Chronic hepatitis C virus infection associated with dermatomyositis and hepatocellular carcinoma. Chang Gung Med J 2004;27:834-9.
[Google Scholar]
|
| 3. |
McMurray RW, Elbourne K. Hepatitis C virus infection and autoimmunity. Semin Arthritis Rheum 1997;26:689-701.
[Google Scholar]
|
| 4. |
Fong TL, Valinluck B, Govindarajan S, Charboneau F, Adkins RH, Redeker AG. Short-term prednisone therapy affects aminotransferase activity and hepatitis C virus RNA levels in chronic hepatitis C. Gastroenterology 1994;107:196-9.
[Google Scholar]
|
| 5. |
Marie I, Menard JF, Hatron PY, Hachulla E, Mouthon L, Tiev K, et al. Intravenous immunoglobulins for steroid-refractory esophageal involvement related to polymyositis and dermatomyositis: A series of 73 patients. Arthritis Care Res (Hoboken) 2010;62:1748-55.
[Google Scholar]
|
| 6. |
Issam Beyrouti M, Beyrouti R, Ben Amar M, Frikha F, Beyrouti R, Abid M, et al. Linitis plastica. Presse Med 2007;36(12 Pt 2):1782-6.
[Google Scholar]
|
| 7. |
Terada T. Signet-ring cell carcinoma of the esophagus in dermatomyositis: A case report with immunohistochemical study. J Gastrointest Cancer 2013;44:489-90.
[Google Scholar]
|
Fulltext Views
3,316
PDF downloads
1,728





![[Figure - 1]](#fig_ijdvl_2017_83_5_606_211160_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2017_83_5_606_211160_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2017_83_5_606_211160_f3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2017_83_5_606_211160_f4.jpg){kind=link}
![[Figure - 5]](#fig_ijdvl_2017_83_5_606_211160_f5.jpg){kind=link}
![[Figure - 6]](#fig_ijdvl_2017_83_5_606_211160_f6.jpg){kind=link}
![[Figure - 7]](#fig_ijdvl_2017_83_5_606_211160_f7.jpg){kind=link}
![[Figure - 8]](#fig_ijdvl_2017_83_5_606_211160_f8.jpg){kind=link}
![[Figure - 9]](#fig_ijdvl_2017_83_5_606_211160_f9.jpg){kind=link}