
Translate this page into:
Dermoscopic characterisation of angiolymphoid hyperplasia in skin of colour: A case series of six patients with review of literature
-
Received: ,
Accepted: ,
How to cite this article: Chauhan P, Vinay K, Jindal R, Goyal P, Meena, DK. Dermoscopic characterisation of angiolymphoid hyperplasia in skin of colour: A case series of six patients with review of literature. Indian J Dermatol Venereol Leprol. doi: 10.25259/IJDVL_1044_2023
Dear Editor,
Angiolymphoid hyperplasia with eosinophilia (ALHE) is a rare, chronic, benign vascular proliferation of unknown aetiology, which typically presents as solitary or multiple pink-to-red papules or nodules on head or neck areas.1,2 It is usually asymptomatic, however, itching, bleeding and tenderness may be associated. Given the predilection for involvement of exposed sites and associated symptoms, if any, ALHE can be a distressing disorder for patients. Dermoscopy can be a useful diagnostic modality for this uncommonly encountered disorder, considering the rapid and non-invasive nature of the procedure. There is a shortage of literature on dermoscopy of ALHE in the skin of colour; findings are found to vary from those described in lighter skin phenotypes.3 In the current study, we retrospectively analysed the clinical profile of six biopsy-proven cases of ALHE with skin type IV–V and reviewed dermoscopic findings in a total of 17 lesions. Dermoscopy images were taken using DermLite™ DL4 (3Gen, San Juan Capistrano, CA, USA) at ×10 magnification. Dermoscopic findings were analysed for the presence of lines, dots, clod, structureless zone, vessels or else (according to International Dermoscopy Society criteria (IDS) for skin tumours for skin of colour).3 Presence of findings not delineated in the IDS criteria were recorded under “other relevant findings”.
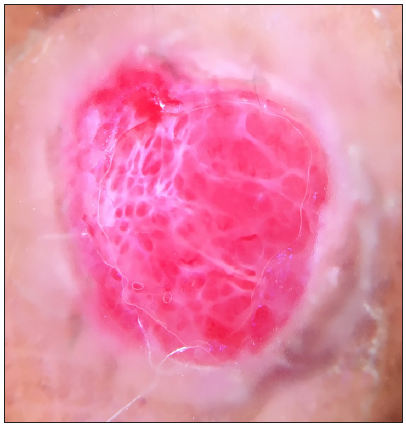
All six patients were female (average age 39.1 years, range 24–50 years, Fitzpatrick’s phototype IV: 1, V: 5). Clinical history revealed eight lesions to be of recent onset (< 6 months) and nine lesions to be present ≥ 6 months (late lesions). None of the patients had any history of trauma or any other associations. Investigations of all patients, including eosinophil levels and renal function tests, were within normal limits. The most frequent findings were the presence of more than one type or polymorphic vessels (most commonly a combination of dotted, linear, and curved/serpentine), with polarisations specific white structures (white structureless areas, white lines, white dots), and clods (red-purple lacunes) [Table 1]. The other notable dermoscopic findings in the present analysis were brown structures (structureless zone, dots), pink structureless zones either focally or as a diffuse background, pigment network and erosions (seen as red-brown dots/globules). In addition, the peripheral rim of pigmentation and scales (most commonly patchy white) were seen. [Figures 1a–d and 2a–e]
| S. No | Dermoscopic findings | Number of lesions (%, total lesions-17) |
|---|---|---|
| 1. |
Vessels Polymorphic
Monomorphic
|
16 (94.1%) 15 9 4 2 1 1 |
| 2. |
Lines White Brown Pigment network |
15 (88.2) 1 (5.8) 7 (41.1) |
| 3. |
Dots White Brown |
15 (88.2) 8 (47.0) |
| 4. |
Structureless zone White Brown Orange Pink
|
10 (58.8) 10 (58.8) 1 (5.8) 10 (58.8) 6 4 |
| 5. | Clods (red-purple lacuna) | 12 (70.5) |
| 6. | Erosions | 3 (17.6) |
| 7. |
Other relevant findings (not in International Dermoscopy Society criteria) Pigmentation structures
Scales
|
10 (58.8) 16 (94.1%) 15 (with Y in 1, B in 2) 2 (with W in 1, B in 1) 3 |

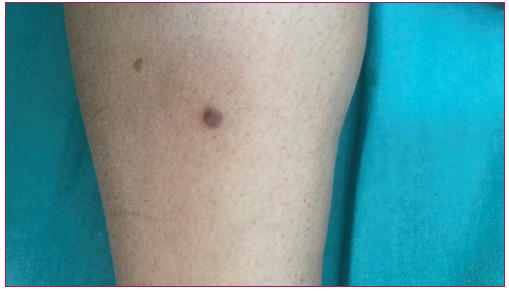
- Clinical image with corresponding multiple erythematous papulonodular lesions over the scalp of a female patient 1.
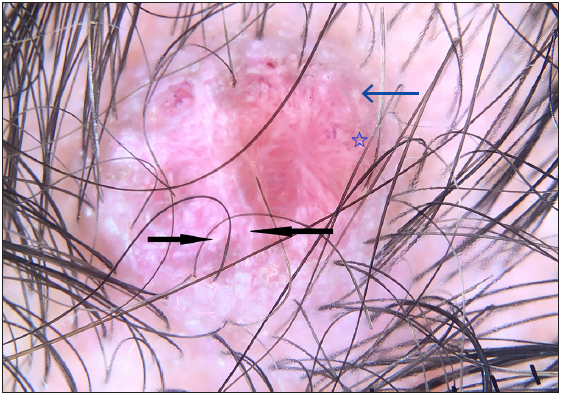
- Dermoscopy of lesion showing similar findings of polymorphic vessels, white structures [white structureless zones, white lines (black arrow), dots] (blue arrow), brown structureless zone (blue star), peripheral rim of pigmentation (DermLite DL4; 3Gen; San Juan Capistrano, California, USA, noncontact polarised mode, 10x magnification).

- Clinical image of another patient with corresponding erythematous plaque, nodule and postinflammatory hyperpigmentation over concha and antihelix of left ear of the patient 2.
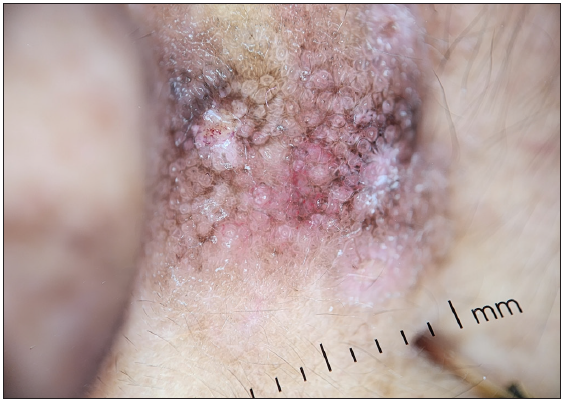
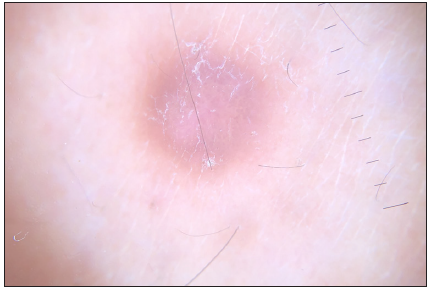
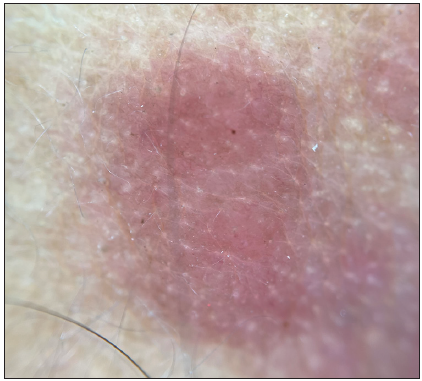
- Dermoscopic examination showing a prominent pigment network, brown dots, along with vessels, and white structures (DermLite DL4; 3Gen; San Juan Capistrano, California, USA, noncontact polarised mode, 10x magnification).

- Clinical image of the third patient of angiolymphoid hyperplasia with eosinophilia (ALHE).

- Dermoscopy examination showing clods (red-purple lacunes, blue arrow), polarising white lines (black arrow), and vessels with a peripheral rim of pigmentation (blue star) seen (DermLite DL4; 3Gen; San Juan Capistrano, California, USA, noncontact polarised mode, 10x magnification).
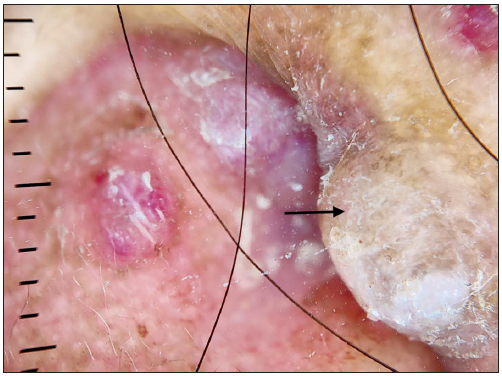
- Late lesion (black arrow) of the same patient 3 showing white structures, pigmentation structures with absence of clods (DermLite DL4; 3Gen; San Juan Capistrano, California, USA, noncontact polarised mode, 10x magnification).

- Clinical image of the fourth angiolymphoid hyperplasia with eosinophilia patient.
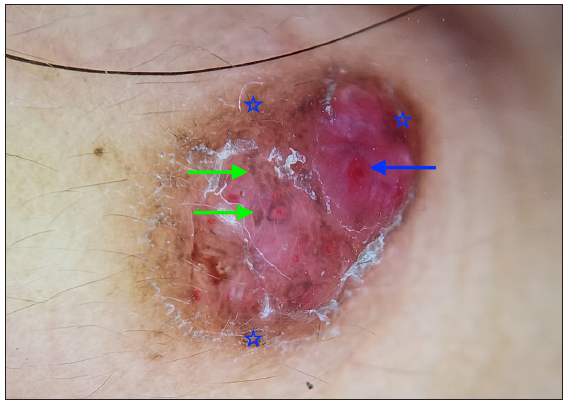
- Dermoscopy showing clods (red-purple lacunes, blue arrow), white scale, and pigmentation structures (green arrow) seen in dermoscopy of another patient. Note the peripheral rim of pigmentation (blue star). (DermLite DL4; 3Gen; San Juan Capistrano, California, USA, noncontact polarised mode, 10x magnification).
Literature on dermoscopy of ALHE is limited to a handful of reports [Tables 2 and 3]. Of a total of 9 cases of dermoscopy of ALHE described hitherto in the literature, only one was in skin of colour. Previous reports have reported red-to-reddish purple lacunae, polymorphic vessels, and white structures over a red-to-pink background in dermoscopy of ALHE.4–7 The findings in the present study align with those described earlier. However, we found polarisation-specific white areas and pigmentation structures to be prominent features, apart from vessels and red lacunae. On dermoscopic-histological correlation, the presence of vessels, clods (red-purple lacunes), and pink background could represent a combination of underlying vascular proliferation with plump endothelial cells, intraluminal erythrocytes and haemorrhage, whereas polarisation-specific white structures might be due to underlying stromal fibrosis and alteration in collagen orientation secondary to vascular proliferation. The pigmentation structures in brown structureless zones/dots/lines, peripheral rim of hyperpigmentation, and pigment network could be due to pigmented skin phototype (IV-V). The presence of peripheral rim of hyperpigmentation, also seen in dermatofibroma, has been linked to trauma as an underlying etiological factor.2 However, no such history was elicited in our patients. We compared the dermoscopic findings between early and late lesions, which revealed more clods, red or purple and erosions in the former. In contrast, late lesions had brown structures (structureless zones, lines), pigment networks, white lines and white dots more frequently. This corroborates with the histological spectrum of ALHE, which varies according to the stage of the lesion, with vascular components more prominent in early lesions and later lesions showing inflammation around mature smaller endothelial cells and stromal fibrosis.
| Author (Year of publication) | Number of cases | Age (years)/sex, skin type | Location of the lesions | Clinical history/morphology | History of trauma/associations |
Dermoscopic setting (polarisation or not/magnification) |
|---|---|---|---|---|---|---|
|
Rodriguez Lomba, et al.5 2016 |
2 |
45, Male, NS 17, female |
The inner aspect of the left thigh Front of neck |
Asymptomatic pink-coloured nodule Asymptomatic, multiple nodules |
NS NS |
polarised/NS polarised/NS |
| Santosa C, et al.7 2019 | 1 |
55, male, NS |
Nose | Solitary, 0.5 cm nodule with a solitary ulcer. History of bleeding. | NS | NS/NS |
| Baştuğ NB, et al.2 2019 | 2 |
40, female, NS 60, female, NS |
Frontotemporal area Periauricular region |
Pink-to-red grouped nodules, rim of brown dots, history of bleeding present There are few pinkish nodules and a history of bleeding after trauma |
NS | Non-polarised/NS |
| Zhang LW, et al.6 2019 | 1 | 24, male, NS | Scalp | Multiple, asymptomatic, dome-shaped papules | NS | NS/NS |
| Kalantri M, et al.1 2020 | 1 | 25, female, NS | Scalp | Multiple, asymptomatic erythematous to skin coloured, discrete and grouped, dome-shaped papules and nodules | Pregnancy | Polarised/x200 |
| Akay BN, et al.4 2021 | 2 |
46, female, NS 35, male, NS |
Right posterior auricular area Left preauricular area |
Asymptomatic multinodular reddish lesion Pruritic, multiple, pink-coloured papules |
NS | NS/NS |
NS: not specified
| Study | Dermoscopic findings (prevalence in percentage) | Corresponding terminology based on the International Dermoscopy Society consensus paper |
|---|---|---|
|
Rodriguez-Lomba, et al.5 2016 |
|
|
| Santosa C, et al.7 2019 |
|
|
| Baştuğ NB, et al.2 2019 |
|
|
| Zhang LW, et al.6 2019 |
|
|
| Kalantri M, et al.1 2020 |
|
|
| Akay BN, et al.4 2021 |
|
|
NA: not applicable
ALHE can act as a diagnostic challenge with a long list of differentials, including pyogenic granuloma, dermatofibroma, pseudolymphoma and Kaposi sarcoma, to name a few [Figures 3a–f]. The presence of a combination of the polymorphic vessels, white and brown structures, clods (red-purple lacunes) with pink structureless zones and erosions could be helpful dermoscopic clues in the diagnosis of ALHE when faced with red-to-pink papulonodules, although more studies with a higher number of patients are needed to affirm findings of the present study.

- Clinical image of a patient with pyogenic granuloma.
- Dermoscopy of pyogenic granuloma showing multiple red lacune, homogenous red zone with interconnected perpendicular white lines (also called rail lines), subtle surrounding scale (called collarette), and vessels in the periphery with conspicuous absence of pigmentation structures (DermLite DL4; 3Gen; San Juan Capistrano, California, USA, noncontact polarised mode, 10x magnification).
- Clinical image of a patient with dermatofibroma.
- Dermatofibroma showing central white structureless zone with peripheral homogeneous pigmentation on dermoscopy (DermLite DL4; 3Gen; San Juan Capistrano, California, USA, noncontact polarised mode, 10x magnification).

- Clinical image of a patient with pseudolymphoma.
- Dermoscopy of pseudolymphoma showing homogenous red background, short linear vessels with yellow-white dots representing follicular openings. (DermLite DL4; 3Gen; San Juan Capistrano, California, USA, noncontact polarised mode, 10x magnification).
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript, and no images were manipulated using AI.
References
- Spectrum of dermoscopic pattern in a patient with angiolymphoid hyperplasia with tissue eosinophilia. Indian J Dermatol. 2020;65:556-8.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Angiolymphoid hyperplasia with eosinophilia: Two case reports. Australas J Dermatol. 2019;60:e236-7.
- [CrossRef] [PubMed] [Google Scholar]
- International Dermoscopy Society (IDS) criteria for skin tumors: Validation for skin of color through a delphi expert consensus by the “Imaging in skin of color” IDS task force. Dermatol Pract Concept. 2023;13:e2023067.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Dermoscopic features of two cases of angiolymphoid hyperplasia with eosinophilia and review of the literature. Dermatol Pract Concept. 2021;11:e2021003.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Dermoscopic features in 2 cases of angiolymphoid hyperplasia with eosinophilia. J Am Acad Dermatol. 2016;75:e19-21.
- [CrossRef] [PubMed] [Google Scholar]
- sQuiz your knowledge! Multiple red papules on the scalp. Eur J Dermatol. 2019;29:577-8.
- [CrossRef] [PubMed] [Google Scholar]
- Angiolymphoid hyperplasia with eosinophilia with clinical pictures of keratoacanthoma: A rare case report. Clin Case Rep. 2018;7:189-92.
- [CrossRef] [PubMed] [Google Scholar]




