
Translate this page into:
Dermoscopic features in a case of chondroid syringoma
Corresponding author: Dr. Biswanath Behera, Department of Dermatology and Venereology, AIIMS, Bhubaneswar - 751 019, Odisha, India. biswanathbehera61@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Palit A, Sethy M, Nayak AK, Ayyanar P, Behera B. Dermoscopic features in a case of chondroid syringoma. Indian J Dermatol Venereol Leprol 2021;87:89-92.
Sir,
A 42-year-old man with skin type IV presented with a one and half year history of a slow-growing, asymptomatic swelling on the right side of the upper lip. He denied any history of spontaneous ulceration or discharge from the lesion. Cutaneous examination revealed a solitary 1 × 1 cm firm, non-tender skin-colored to erythematous nodule on the right side of the upper lip [Figure 1]. The surface of the nodule was uneven and showed areas of brown pigmentation. There was no lymphadenopathy; other general and systemic examinations were within normal limits. Dermoscopic examination under polarized mode (Dermlite DL4, 10 × magnification) revealed white structureless area, milia-like cyst, irregular brown blotches with a few white lines, an erythematous rim at the periphery and linear curved vessels [Figure 2]. Differential diagnoses of nodular hidradenoma, solitary trichoepithelioma and nodular basal cell carcinoma were considered. Histopathology showed proliferation of epithelial cells arranged in nests, irregular tubulo-alveolar and ductal structures in a myxoid to fibromyxoid matrix. Apocrine decapitation secretion, cystic dilatation, clear cell change, mature adipocytes and keratocysts were evident at places [Figure 3a and b]. There was no evidence of any infiltrative growth pattern, pleomorphism, excessive/ abnormal mitotic activity or tumor necrosis suggestive of malignant change. On immunohistochemistry, the outer epithelial and stromal cells were positive for vimentin and the inner epithelial cells for carcinoembryonic antigen and epithelial membrane antigen [Figure 3c and d]. A diagnosis of chondroid syringoma was made.

- Solitary skin-colored to erythematous nodule on the right side of the upper lip
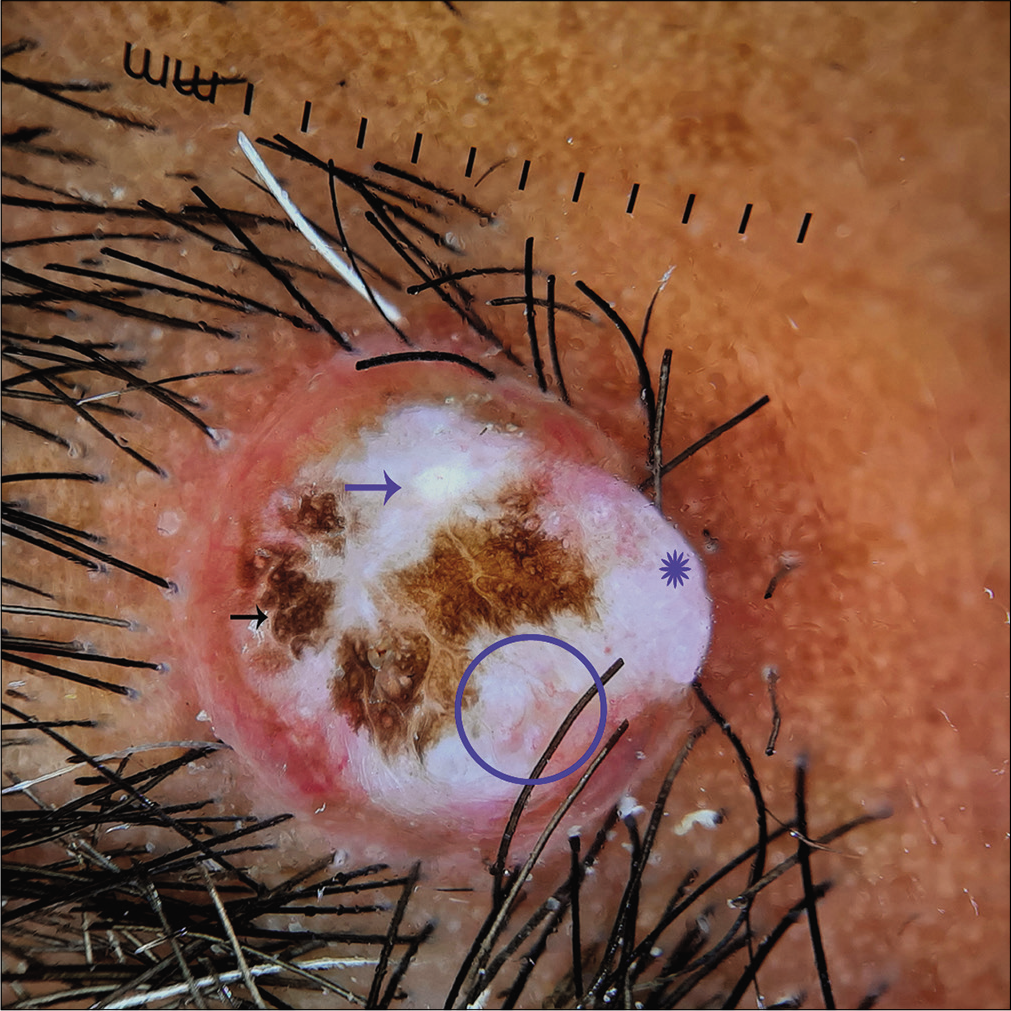
- Dermoscopy under polarized mode (Dermlite DL4, ×10) showing white structureless area (Asterix), milia-like cyst (blue arrow), irregular brown blotches with a few white lines (black arrow), peripheral erythematous rim and linear curved vessels (circle)
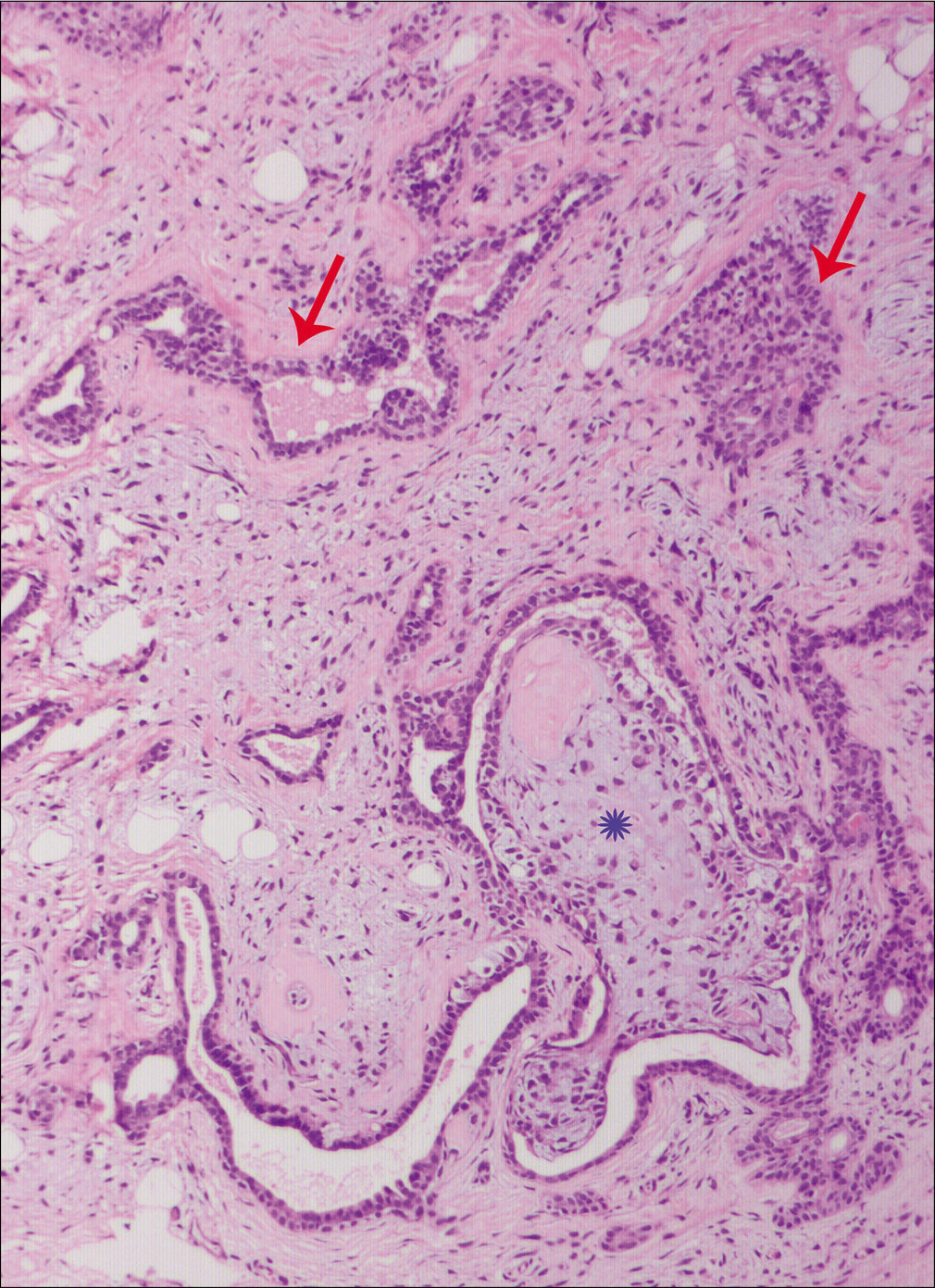
- The proliferating epithelial cells arranged in nests, irregular tubulo-alveolar and ductal structures (red arrows) and lined by two layers of epithelial cells in a myxoid to fibromyxoid matrix (Asterix, H and E, ×100)
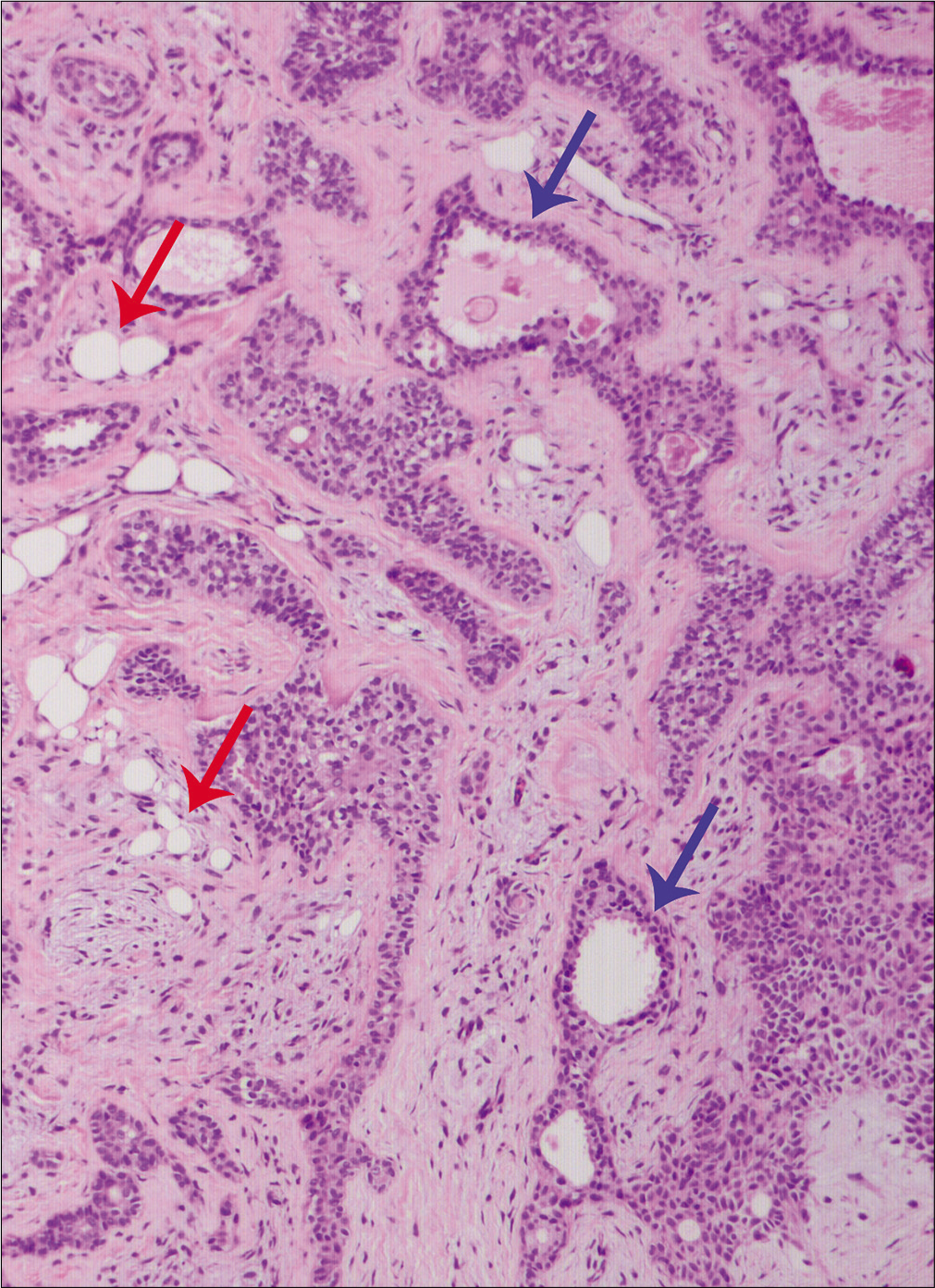
- Apocrine decapitation secretion (blue arrows) and mature fat cells (red arrows, H and E, ×100)
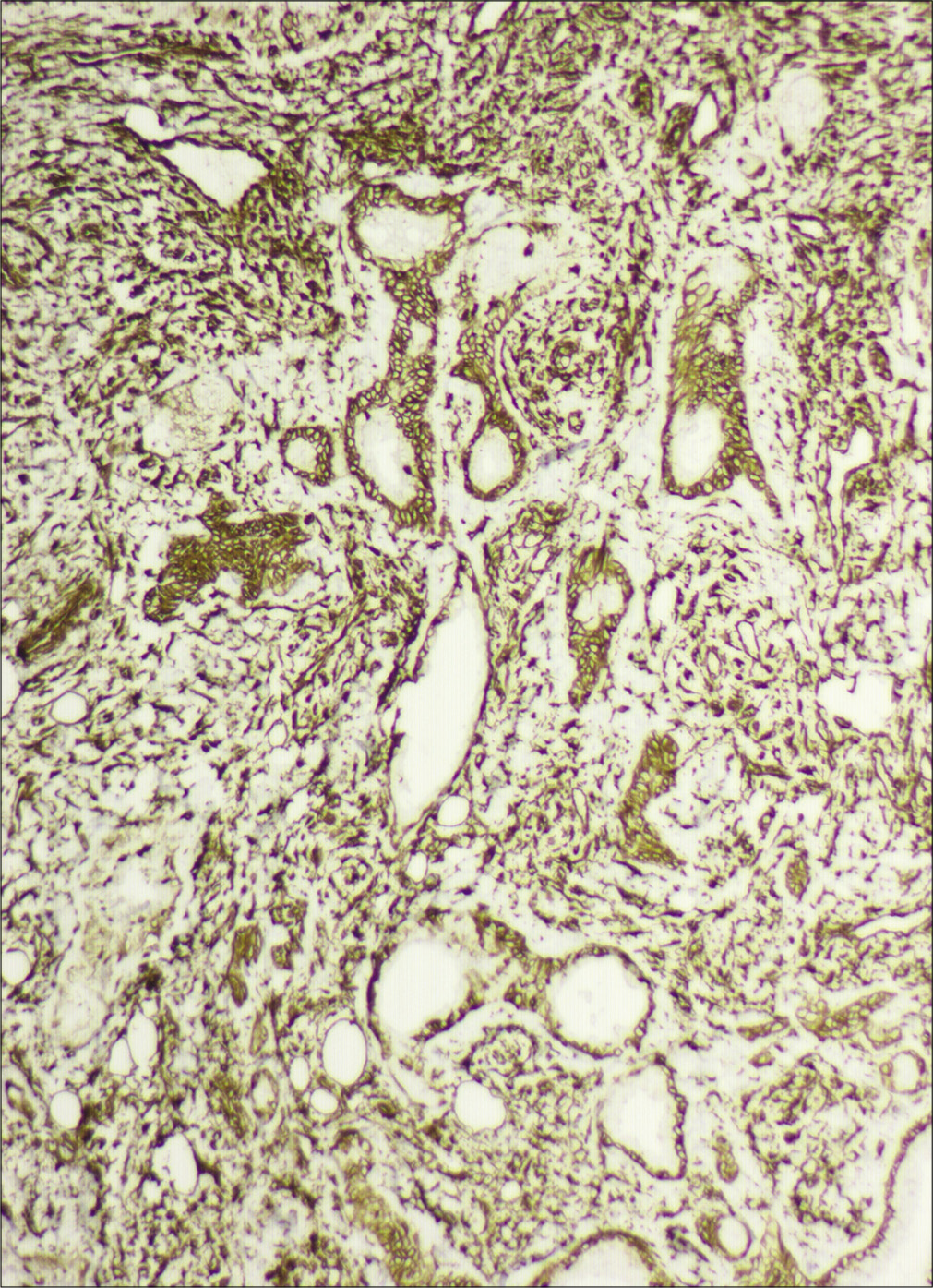
- Immunohistochemistry showing vimentin positivity (IHC, ×100)
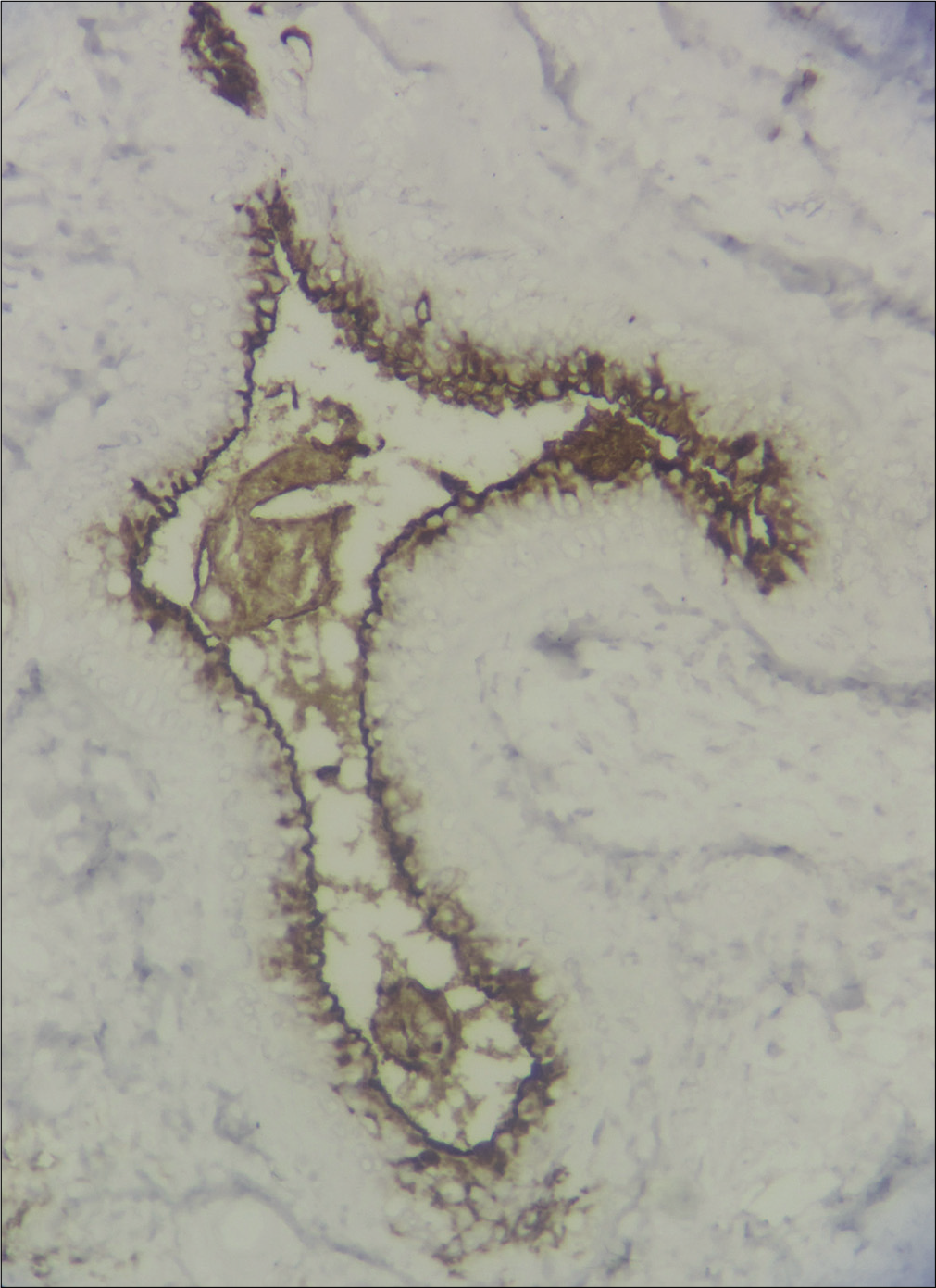
- Immunohistochemistry showing carcino-embryogenic antigen positivity (IHC, ×400)
Cutaneous chondroid syringoma is a rare, benign, cutaneous sweat gland neoplasm that commonly occurs in the head and neck region of middle-aged men.1 It usually presents as a solitary, well-circumscribed, asymptomatic, firm to hard, slow-growing, lobulated nodule of size varying from 0.5 cm to 3 cm. The color of the lesion varies from skin-colored to erythematous to bluish.1 A consistent feature of chondroid syringoma is the lack of ulceration. Clinical diagnosis of chondroid syringoma is relatively difficult as it mimics other cutaneous tumors and cysts like basal cell carcinoma, hidradenoma, pilomatrixoma, sebaceous cyst and steatocystoma simplex.1
Dermoscopic examination as a supportive diagnostic tool has been used in various cutaneous tumors. The dermoscopic pattern and features displayed by a cutaneous neoplasm depend upon the cell of origin, its growth pattern, nature of the stroma, the thickness of overlying epidermis, type of light used (polarized versus non-polarized) and lastly and most importantly, the color of skin of the patient. Dermoscopic features of chondroid syringoma are rarely reported in literature and include homogenous white-blue color pattern.1 The predominant dermoscopic features in the index case were a white structureless area, milia-like cyst and peripheral linear curved vessels. The absence of blue color, in the present case, is due to the lack of dominant chondroid stroma. Instead, a myxoid to fibromyxoid stroma dominated the histopathologic picture. The dermoscopic feature of milia-like cyst that corresponds to the dermal keratocyst, points to the follicular-sebaceous-apocrine origin of the tumor. Two types of milia-like cysts have been described, i.e., cloudy and starry. It is not a specific feature of any particular cutaneous neoplasm and has been described in seborrheic keratosis, solar lentigo, congenital melanocytic nevi, trichoepithelioma, trichoblastoma, basal cell carcinoma and malignant melanoma.2-5 In seborrheic keratosis, it corresponds histologically to the epidermal horn cyst, and is better visualized by a non-polarized dermoscope. In trichoepithelioma and trichoblastoma, it histopathologically corresponds to the dermal keratocyst and is better visualized by a polarized dermoscope, as in our case. The white structureless area corresponds to the fibrous stroma, the brown blotch to the increased epidermal pigmentation and peripheral erythema to the increased vascularity. The dermoscopic differential diagnoses in our case included basal cell carcinoma, nodular hidradenoma, trichoepithelioma and pilomatrixoma. Absence of any of the classic basal cell carcinoma-associated pigmented structures in our patient with a skin type IV makes basal cell carcinoma a lesser possibility as most of the basal cell carcinomas in dark skin phototype are pigmented. The most common dermoscopic pattern described for nodular hidradenoma is a homogenous area of varying color, white and vascular structures. The homogenous areas vary from pinkish, bluish, pink-bluish to brown, depending upon the color of the lesion. The associated vascular structures are arborizing telangiectasias, polymorphous atypical vessels and linear irregular vessels.6 The dermoscopic picture of a trichoepithelioma demonstrates shiny white areas/background and milia-like cysts along with small, thin, in-focus arborizing vessels. Pilomatrixoma is characterized by the presence of irregularly distributed white and/or yellow homogeneous area, white streaks, reddish homogeneous areas, hairpin vessels and linear irregular vessels.6
Due to the lack of certainty in the clinical diagnosis, histopathological examination becomes mandatory for the diagnosis of chondroid syringoma. A well-circumscribed multilobulated tumor mass, separated by fibrous septa, situated in the deep dermis and/or subcutaneous tissue, is the feature of chondroid syringoma . The stroma can have a variable appearance. Characteristically, it has a homogeneous, bluish, chondroid appearance but can be myxoid or densely collagenous, eosinophilic and hyalinized. The epithelial component is composed of cuboidal or polygonal cells distributed singly, in cords and nests, or as irregular tubuloalveolar and ductal structures.1 Rarely, in doubtful cases, immunohistochemistry may be needed for the diagnosis. The inner epithelial cell layer stains positive for high and low molecular weight keratin (AE1/AE3), epithelial membrane antigen, carcinoembryogenic antigen and gross cystic disease fluid protein-15, while the outer cells express vimentin, S-100 protein and sometimes smooth muscle antigen and muscle-specific actin. Stromal cells stain positive for vimentin and S-100 protein. The treatment of choice for chondroid syringoma is surgical excision.1
In conclusion, we are reporting new dermoscopic features such as a white structureless area, milia-like cysts and linear curved vessels, in a case of chondroid syringoma, and hopefully a larger case series could delineate the specific dermoscopic features in the future.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given his consent for his images and other clinical information to be reported in the journal. The patient understands that name and initials will not be published and due efforts will be made to conceal identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Chondroid syringoma: A clinical and histological review of eight cases. Actas Dermosifiliogr. 2006;97:573-7.
- [CrossRef] [Google Scholar]
- Cloudy and starry milia-like cysts: How well do they distinguish seborrheic keratoses from malignant melanomas? J Eur Acad Dermatol Venereol. 2011;25:1222-4.
- [CrossRef] [PubMed] [Google Scholar]
- Multiple familial trichoepithelioma: Confirmation via dermoscopy. Dermatol Pract Concept. 2016;6:51-4.
- [CrossRef] [PubMed] [Google Scholar]
- Dermoscopic findings in trichoblastoma. Actas Dermosifiliogr. 2015;106:e45-8.
- [CrossRef] [Google Scholar]
- Dermoscopic yellow structures in basal cell carcinoma. J Eur Acad Dermatol Venereol. 2014;28:651-4.
- [CrossRef] [PubMed] [Google Scholar]




