Translate this page into:
Dermoscopic features of various stages of lichen planus
Correspondence Address:
Tishya Singh
OPD-17, Department of Dermatology and Venereology, Hinduhridaysamrat Balasaheb Thackeray Medical College and Dr. RN Cooper Hospital, Mumbai, Maharashtra
India
| How to cite this article: Makhecha M, Singh T, Malladi N, Rambhia K. Dermoscopic features of various stages of lichen planus. Indian J Dermatol Venereol Leprol 2020;86:191-194 |
Sir,
Lichen planus is a papulosquamous disorder that is known to cause post-inflammatory hyperpigmentation which can be prevented if diagnosed early and effective treatment is instituted in time.
Dermoscopy recognizes even the subtle morphological changes in lichen planus. We conducted a study of the clinical and dermoscopic features of various stages of lichen planus. This was a cross-sectional single-center descriptive study performed over a period of 3 months at Dr. R.N Cooper Hospital, Mumbai. This study included 111 patients with a diagnosis of classical lichen planus. These patients were not on any topical or systemic treatment for past 6 months.
Each patient was subjected to detailed history and examination. Diagnosis of lichen planus was made clinically and was confirmed histopathologically. Dermoscopic images of the representative lesions from each patient were taken using a manual dermoscope (HEINE DELTA 20 Plus) attached to a digital camera after applying ultrasound gel.
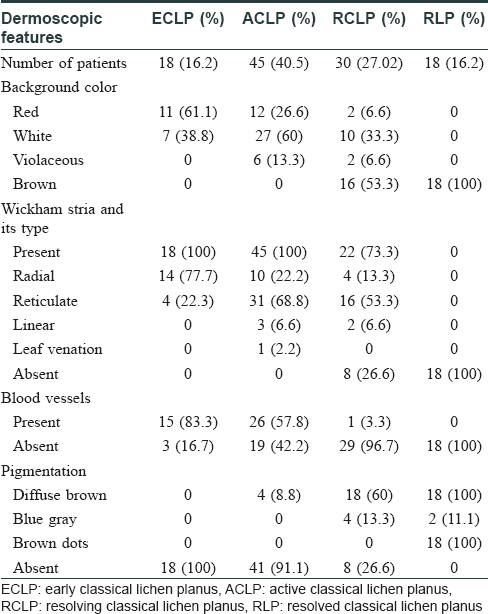
Variables used in the dermoscopic evaluation were background color (red, white, violaceous and brown), blood vessels (presence or absence), Wickham striae (presence or absence), type of Wickham striae (radial, reticulate, leaf venation and linear) and pigmentation (diffuse brown pigmentation, blue-gray and brown dots).
Authors propose classification of classical lichen planus into four different stages: early classical lichen planus, active classical lichen planus, resolving classical lichen planus and resolved classical lichen planus opposed to the earlier one which had only early classical lichen planus, active classical lichen planus and resolved classical lichen planus type.[1],[2] We found a subtle difference in last two types with respect to clinical, dermoscopic and histopathological features.
Collected data was analyzed using Microsoft Office Excel 2007 and SPSS version 16.0. The data was presented as frequency and proportions [Table - 1].
Early classical lichen planus [Figure - 1]: The dermoscopic findings of early classical lichen planus revealed a red background in most patients and Wickham striae in all patients. The red background corresponds to active inflammation and dilated blood vessels. Wickham striae was observed in radial pattern in maximum patients corresponding to the early proliferation of epidermis as beaded hypergranulosis. This is in accordance with the study by Haldar and Khopkar.[1] No pigmentation was seen because of the absence of melanophages.
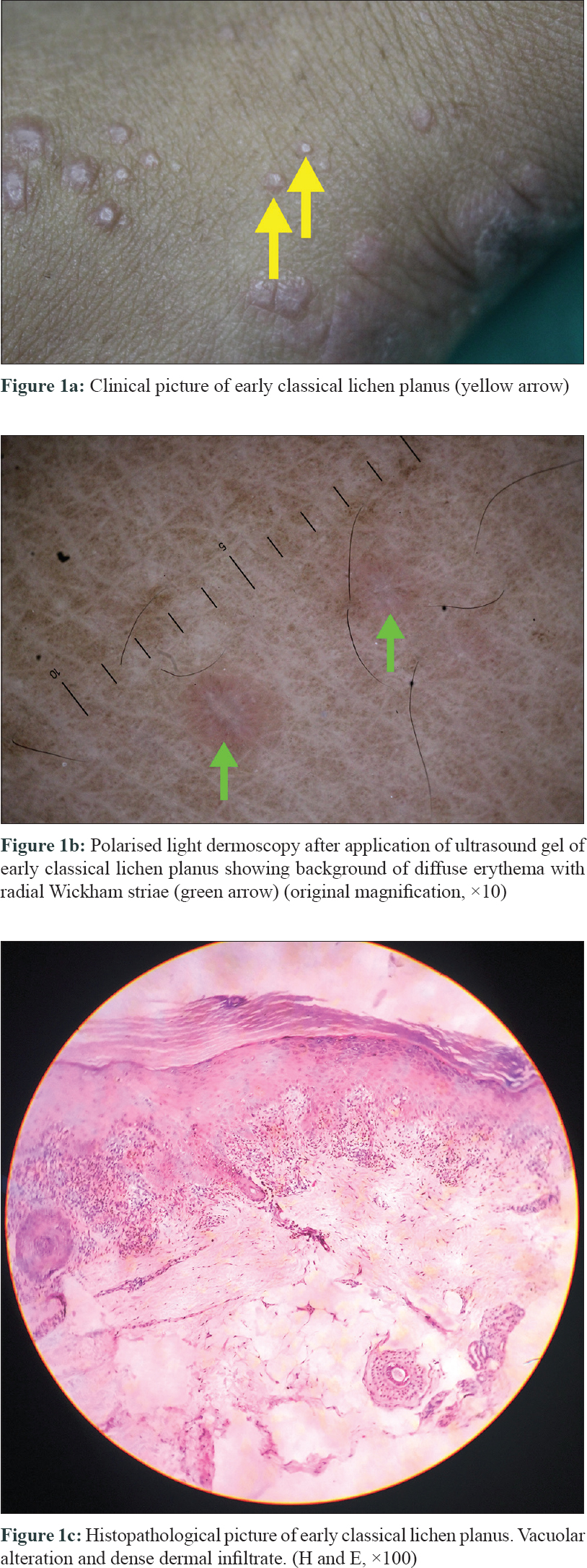 |
| Figure 1: |
Active classical lichen planus [Figure - 2]: The progression of the disease is associated with dermoscopic findings of white background in some lesions and structured white areas called Wickham striae which were present in all the lesions, correlating with epidermal proliferation in the form of wedge-shaped hypergranulosis and irregular acanthosis. This epidermal proliferation further led to reduced visualization of blood vessels. Diffuse brown pigmentation seen in a few patients is suggestive of epidermal pigmentation.[3]
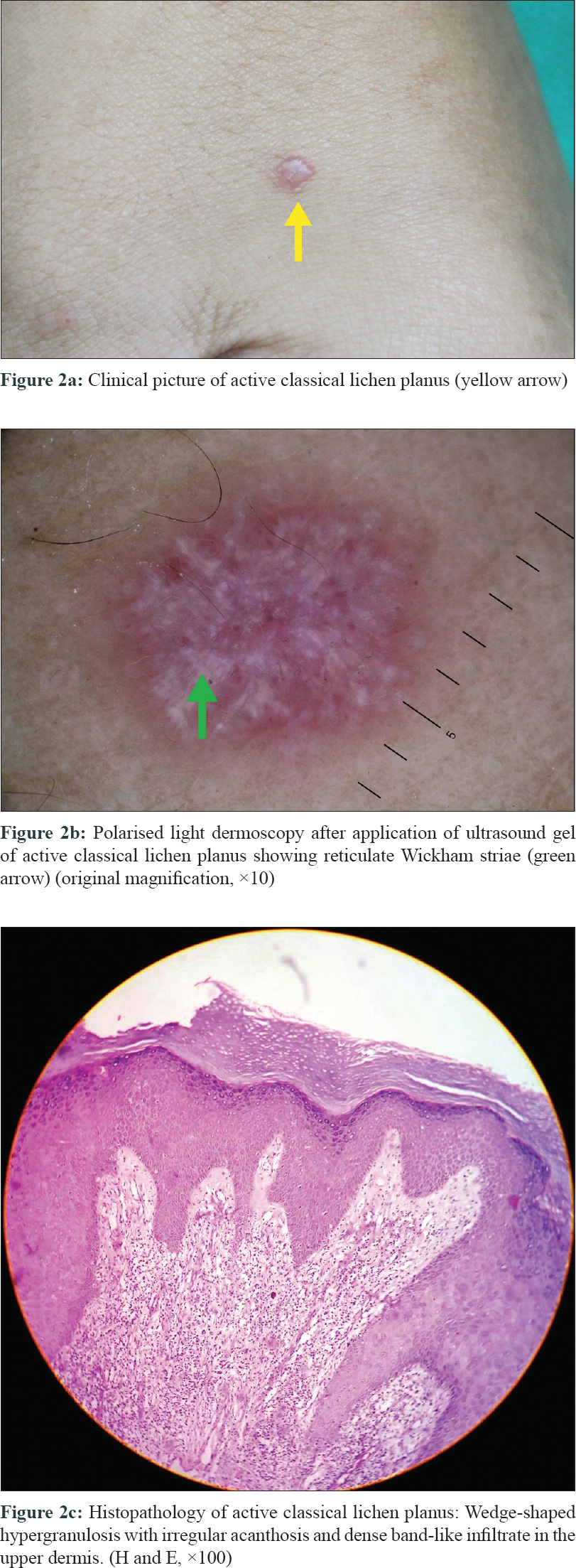 |
| Figure 2: |
Resolving classical lichen planus [Figure - 3]: As the inflammation reduces in resolving lesions, the finding of presence of persisting blood vessel was noted in a single patient. The decreasing inflammation further leads to reduction in compensatory proliferation of keratinocytes, manifesting as reduction in thickness of lesions clinically and dermoscopically as reduction in white background.[4] There was increase in brown background secondary to diffuse brown pigmentation of epidermal origin manifesting clinically as postinflammatory hyperpigmentation. A blue-gray pigmentation corresponding to melanophages secondary to melanin incontinence was also visible.[3]
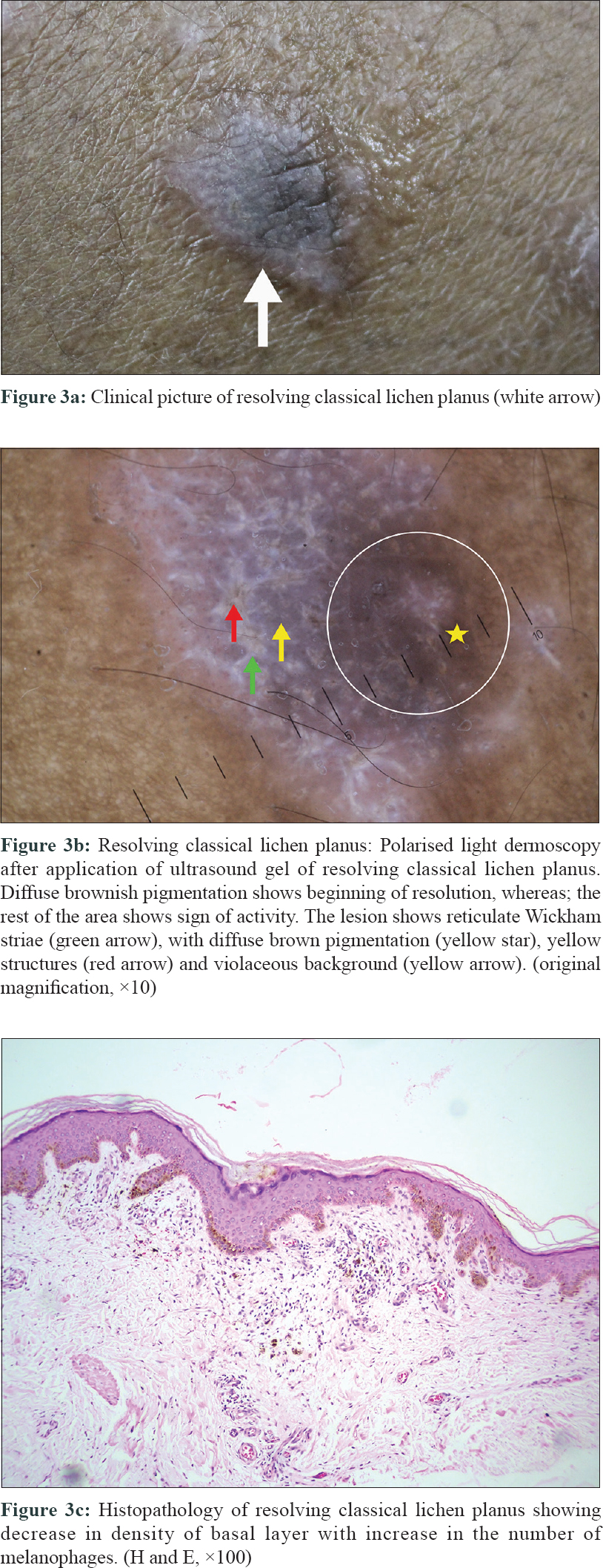 |
| Figure 3: |
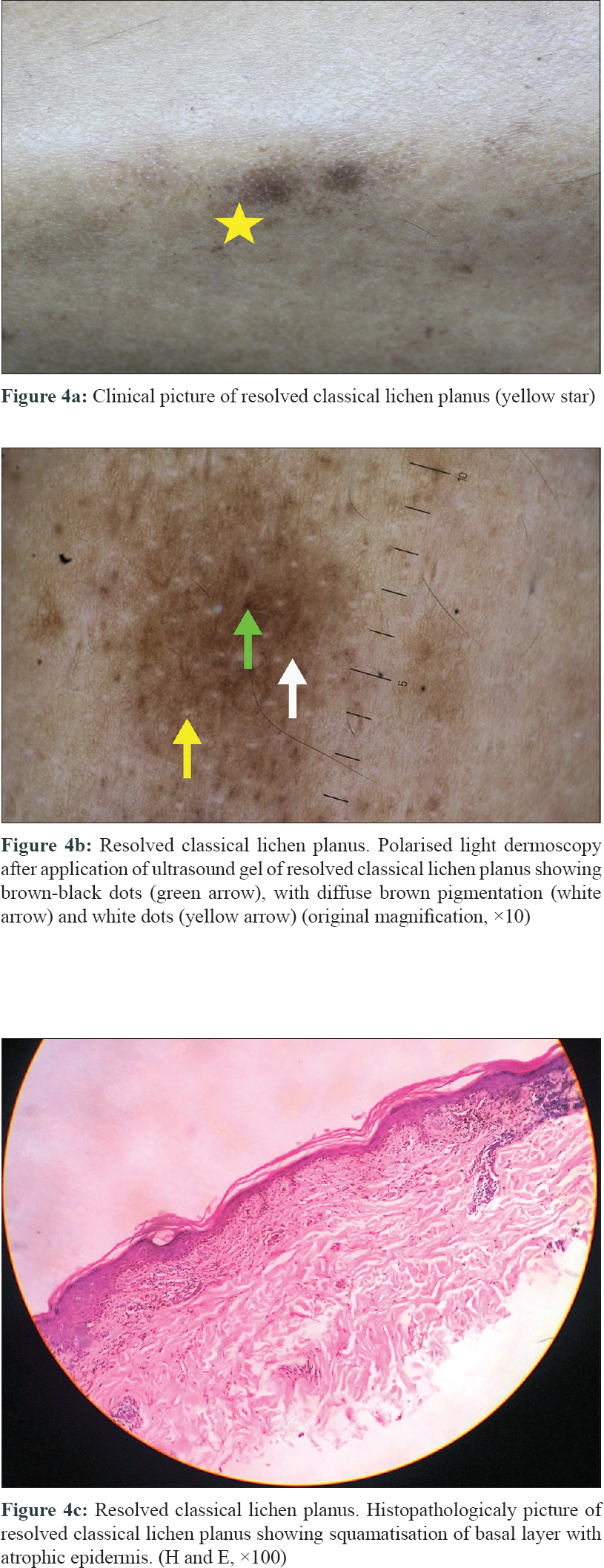
Resolved classical lichen planus [Figure - 4]: There was no erythema or presence of blood vessels with cessation of inflammation and involution of epidermal proliferation. There was also an absence of Wickham striae similar to the study by Güngör et al.[2] We observed that maximum patients had diffuse brown background with fine or coarse gray-blue dots in some patients and brown to brown-black dots of various patterns present in all patients. This finding was better appreciated due to reduced epidermal thickness. Similar results were present in the study by Tan et al.[5] The above findings show that Wickham striae are seen in active lesions and disappear with treatment, but the pigment patterns resist treatment. They can even appear during late stages in spite of treatment. Sparing of creases and white dots were also seen in many patients.
 |
| Figure 4: |
The limitations of this study are a small sample size and the cross-sectional design.
Future prospective studies including large number of patients to observe the evolution of lesions are indicated.
Although classical lichen planus can be easily diagnosed clinically, the need for definite diagnosis of early lesions, thereby targeting the disease process in its initial phase and preventing pigmentary sequelae was addressed in this study. In addition, dermoscopy helps to avoid biopsy, monitor the efficacy of the therapy and gauge the endpoint of treatment.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patients have given their consent for their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Haldar SS, Khopkar U. Dermoscopy of lichen planus. In Lichen Planus. Khopkar U, Valia A, editors. 1st ed. New Delhi: Jaypee; 2013. p. 148-62.
[Google Scholar]
|
| 2. |
Güngör Ş, Topal IO, Göncü EK. Dermoscopic patterns in active and regressive lichen planus and lichen planus variants: A morphological study. Dermatol Pract Concept 2015;5:45-53.
[Google Scholar]
|
| 3. |
Friedman P, Sabban EC, Marcucci C, Peralta R, Cabo H. Dermoscopic findings in different clinical variants of lichen planus. Is dermoscopy useful? Dermatol Pract Concept 2015;5:51-5.
[Google Scholar]
|
| 4. |
Pock L, Jelínková L, Drlík L, Abrhámová S, Vojtechovská S, Sezemská D, et al. Lichen planus pigmentosus-inversus. J Eur Acad Dermatol Venereol 2001;15:452-4.
[Google Scholar]
|
| 5. |
Tan C, Min ZS, Xue Y, Zhu WY. Spectrum of dermoscopic patterns in lichen planus: A case series from China. J Cutan Med Surg 2014;18:28.32.
[Google Scholar]
|
Fulltext Views
17,286
PDF downloads
5,268





![[Table - 1]](#tbl_ijdvl_2020_86_2_191_278142_t5.jpg){kind=link}
![[Figure - 1]](#fig_ijdvl_2020_86_2_191_278142_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2020_86_2_191_278142_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2020_86_2_191_278142_f3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2020_86_2_191_278142_f4.jpg){kind=link}