Translate this page into:
Disseminated cutaneous gout: A rare clinical presentation
2 Department of Clinical Pathology, Uijeongbu St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
Correspondence Address:
Eun Duk Jang
Department of Clinical Pathology, Uijeongbu St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul
Korea
| How to cite this article: Jung HY, Yu DS, Kim JW, Jang ED. Disseminated cutaneous gout: A rare clinical presentation. Indian J Dermatol Venereol Leprol 2016;82:204-205 |
Sir,
Gout is a common systemic disorder caused due to abnormal uric acid metabolism. Uric acid crystallizes and gets deposited in the joints resulting in recurrent arthritis. Chronic cutaneous gout is characterized by firm, erythematous nodules called tophi which are present intradermally or in the subcutis. They usually occur in avascular tissue over the ears, olecranon and pre-patellar bursae, or over acral areas around the joints. [1],[2] We report a case of severe, disseminated cutaneous gout that involved non-articular sites and was associated with sepsis.
A 58-year-old Korean male presented with tender, yellowish-red nodules on both upper and lower extremities since one week, along with fever and malaise. He had a history of chronic gouty arthritis for twenty years. Cutaneous examination revealed multiple, firm, yellowish to red nodules over an erythematous base along both sides of his forearms and legs [Figure - 1]. The lesions were warm and swollen. There was no sign of venous insufficiency. The patient was drowsy but his neurological examination was within normal limits. Laboratory investigations revealed an elevation of all of the following: total leukocyte count with band forms, blood urea nitrogen, serum creatinine and serum potassium levels (suggestive of renal failure). The serum uric acid level was within normal limits. His chest radiograph revealed cardiomegaly. Two deep punch biopsies of the nodules over the left thigh were taken. Gross examination revealed whitish material similar to chalk. Histopathology revealed amorphous, pinkish, crystalline material in the dermis, surrounded by granulomatous inflammation [Figure - 2]. Polarized light microscopy revealed negatively birefringent urate crystals with typical needle - like shapes [Figure - 3]. These findings were consistent with intradermal tophaceous gout. Pseudogout was excluded by the absence of characteristic blue refractive crystals. The patient′s renal function worsened over the next two days despite emergency hemodialysis. Blood culture revealed the presence of Staphylococcus haemolyticus and Staphylococcus epidermidis. He developed sepsis and expired due to ventricular tachycardia.
 |
| Figure 1: (a-d) Multiple yellowish to red nodules with underlying erythema over both forearms and lower legs, involving the peri-articular and non-articular regions |
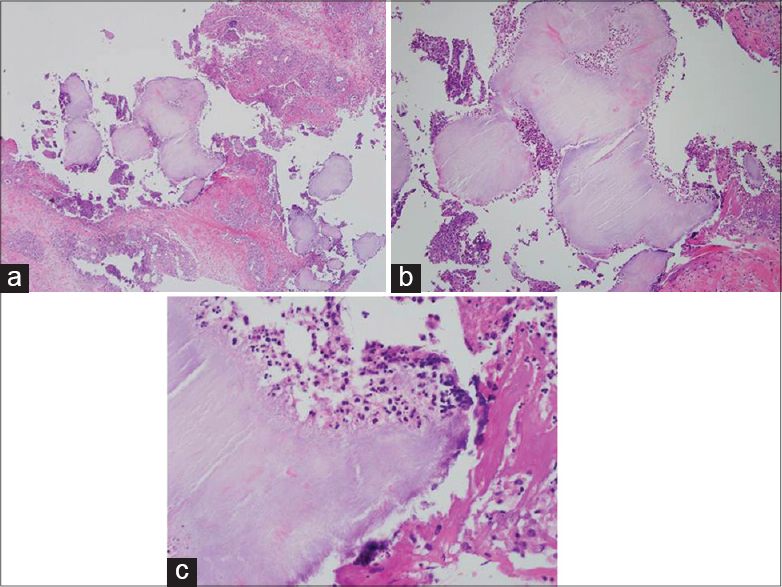 |
| Figure 2: (a-c) Amorphous crystalline material in the dermis, surrounded by granulomatous inflammation (H and E). (a) ×40, (b) ×100, (c) ×400 |
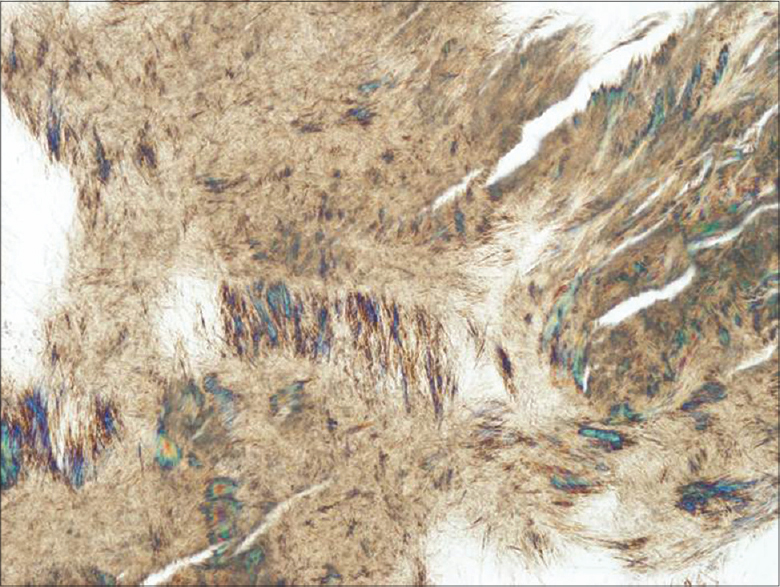 |
| Figure 3: Polarized microscopy revealing multiple needle-like crystals which were negatively birefringent |
There are four stages of gout: asymptomatic hyperuricemia, gouty attack, intercritical period and chronic gouty arthritis. Skin biopsy and appearance of chalk-like material on the open skin and around joints is the gold standard for diagnosis of gout in the chronic stage. Treatment with allopurinol alone, or in combination with colchicine, is effective for the cutaneous and articular manifestations of gout. [1],[2] Atypical forms of tophaceous gout include bullous, fungating and ulcerative gout. Gouty panniculitis has been described in six cases. [3] A variant of cutaneous gout with widespread milia-like eruptions of intradermal tophi is termed as miliarial gout. [4],[5] Miliarial gout is characterized by multiple tiny, painless, white to yellow coloured papules on erythematous areas.
In our patient, the lesions were broadly distributed over both the arms and legs, including non-articular sites. A striking peculiarity of our case is that the lesions resembled nodules rather than tiny milia-like papules. It had a clinical presentation more typical of Sweet′s syndrome or furunculosis. Serum urate levels are usually elevated in gout. However, gout can even occur in the absence of hyperuricemia limiting the diagnostic utility of measuring serum uric acid levels. Although the exact cause of sepsis was unclear in our patient, there is a possibility that cutaneous infection of the gouty nodules may have played a role. The histopathological findings of acute inflammatory cells and abscess formation around the pink amorphous material support this theory.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Falasca GF. Metabolic diseases: Gout. Clin Dermatol 2006;24:498-508.
[Google Scholar]
|
| 2. |
Fam AG, Assaad D. Intradermal urate tophi. J Rheumatol1997;24:1126-31.
[Google Scholar]
|
| 3. |
Snider AA, Barsky S. Gouty panniculitis: A case report and review of the literature. Cutis 2005;76:54-6.
[Google Scholar]
|
| 4. |
Aguayo RS, Baradad M, Soria X, Abal L, Sanmartín V, Egido R, et al. Unilateral milia-type intradermal tophi associated with underlying urate subcutaneous deposition: An uncommon cutaneous presentation of gout. Clin Exp Dermatol 2013;38:622-5.
[Google Scholar]
|
| 5. |
Mireku KA, Burgy JR, Davis LS. Miliarial gout: A rare clinical presentation. J Am Acad Dermatol 2014;71:e17-8.
[Google Scholar]
|
Fulltext Views
6,088
PDF downloads
2,270





![[Figure - 1]](#fig_ijdvl_2016_82_2_204_164220_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2016_82_2_204_164220_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2016_82_2_204_164220_f3.jpg){kind=link}