Translate this page into:
Disseminated discoid lupus erythematosus with a linear lesion on the forearm and hand: A rare presentation and review of literature
2 Department of Dermatology, Burdwan Medical College and Hospital, Burdwan, West Bengal, India
3 Department of Dermatology, All India Institute of Medical Sciences, Bhubaneswar, Odisa, India
4 Department of Surgery, College of Medicine and Sagore Dutta Hospital, Kolkata, India
Correspondence Address:
Abhijit Saha
77/26 Ram Lal Dutta Lane, Rishav Palace, Flat No. 115, Block B, 1st Floor, Uttarpara, Bhadrakali, Hooghly - 712 232, West Bengal
India
| How to cite this article: Saha A, Seth J, Pradhan S, Dattaroy S. Disseminated discoid lupus erythematosus with a linear lesion on the forearm and hand: A rare presentation and review of literature. Indian J Dermatol Venereol Leprol 2017;83:586-589 |
Sir,
Linear cutaneous lupus erythematosus is a rare pattern of lupus erythematosus, mostly reported in children and young adults, with facial predilection. The term linear cutaneous lupus erythematosus was first coined by Abe et al. in 1998.[1] The histopathological findings of such lesions are mostly consistent with discoid lupus erythematosus.[1],[2],[3],[4] We report a case of adult onset disseminated discoid lupus erythematosus, which started as linear cutaneous lupus erythematosus, on the forearm and hand and showed remarkable improvement following treatment. The unique feature of our case lies in the age of onset, the distribution on the forearm, the dissemination of lesions and good response following treatment, which we were unable to find in any previous article.
A 45-year-old woman presented with linear red-colored elevated lesions on the left forearm and hand of 2 years duration. She also complained of other lesions on the left breast, bilateral inguinal area and right side of waist. The lesions first started on the left forearm and gradually involved other areas within 2 years. The patient was asymptomatic, except for intermittent itching. There was no history of photosensitivity. There was no history of any preceding trauma or chronic drug ingestion. There was no history of similar problems in other family members. Her general and systemic examinations were unremarkable. Dermatological examination revealed an erythematous indurated plaque with adherent scaling, along the lines of Blaschko on the inner aspect of the left forearm, extending onto the palm [Figure - 1] with areas of hypopigmentation. The lesions on the left breast, bilateral inguinal areas and the right side of the waist showed additional features of central depigmentation, atrophy, adherent scaling and perilesional hyperpigmentation [Figure - 2] and [Figure - 3].
 |
| Figure 1: Erythematous indurated scaly plaques along the line of Blaschko on the inner aspect of the left forearm and palm |
 |
| Figure 2: Indurated plaque on the left breast, with perilesional hyperpigmentation |
 |
| Figure 3: Atrophic and depigmented lesions on the inguinal region |
Her hematological parameters, liver function tests and renal function tests were within normal limits. Antinuclear antibodies were positive with a homogeneous pattern and titer of 1:80.
Histopathology of the biopsy specimen, both from the plaque on the chest and the linear lesion on the forearm showed hyperkeratosis, epidermal thinning, foci of hydropic degeneration of the basal cell layer and dense perivascular and periappendageal mononuclear cell infiltrate [Figure - 4]. Direct immunofluorescence could not be done due to lack of facilities.
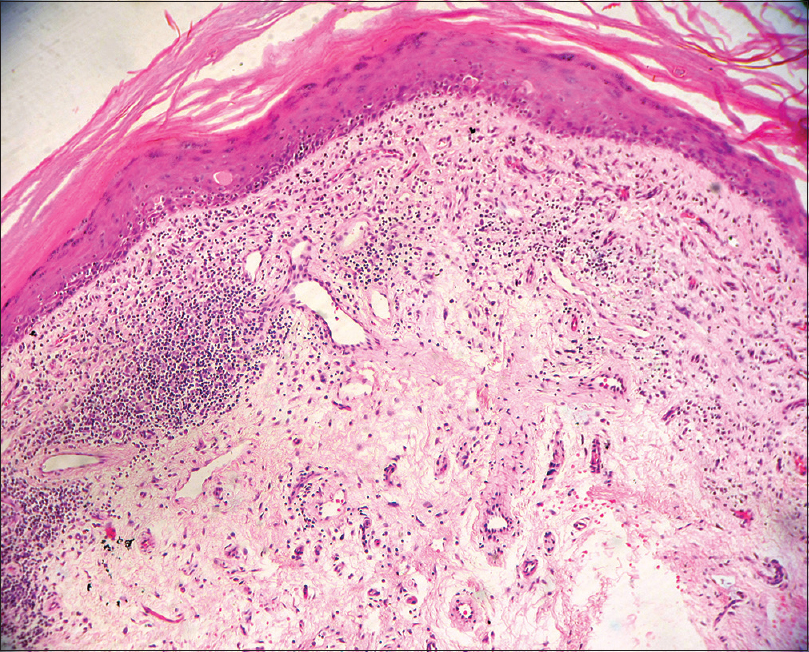 |
| Figure 4: H and E stain (×100) shows hyperkeratosis, epidermal thinning and dense perivascular and periappendageal mononuclear cell infiltrate |
Based on clinical and histopathological findings, the patient was diagnosed to have linear discoid lupus erythematosus with dissemination. She was prescribed oral prednisolone 1 mg/kg/day and topical clobetasol propionate to be applied once daily on the lesions, except on the breast and inguinal region. We prescribed topical tacrolimus for those areas. After ophthalmological examination, hydroxychloroquine (6.5 mg/kg/day) was started. The patient was followed up monthly with gradual tapering of oral prednisolone over 2 months, along with periodic ophthalmological checkup. Topical steroid was discontinued after 1 month, but topical tacrolimus was continued up to 6 months. After 6 months, the lesions improved to a great extent with decrease in erythema, induration and size. [Figure - 5] and [Figure - 6]. Currently, the patient is on oral hydroxychloroquine and sunscreen only.
 |
| Figure 5: Flattened linear lesion on the forearm following treatment |
 |
| Figure 6: Residual atrophic lesion on the left breast following treatment |
Linear involvement in cutaneous lupus erythematosus along the lines of Blaschko is extremely rare. It might be the presenting feature in discoid lupus erythematosus, bullous lupus erythematosus, tumid lupus erythematosus or subacute lupus erythematosus; among which, the most commonly reported form is linear discoid lupus erythematosus.[4] The lupus erythematosus lesions follow lines of Blaschko, which represents pathways of epidermal cell migration and proliferation during fetal development and reflects the existence of genetic mosaicism of keratinocytes.[5]
Most of the reported cases of linear cutaneous lupus erythematosus were in children, with only few cases described in adults.[3],[6] The lesions of linear cutaneous lupus erythematosus have a facial predilection and less frequently can involve the limb and trunk.[6] Neither photosensitivity nor progression to systemic lupus erythematosus is observed. Antinuclear antibodies are usually negative or slightly positive in cases of linear cutaneous lupus erythematosus.[7] In the index case, it was positive with a lower titer. Histopathological features of linear cutaneous lupus erythematosus are usually consistent with features of discoid lupus erythematosus; such as hyperkeratosis, atrophy of the epidermis, hydropic degeneration of the basal cell layer in the epidermis, dense perivascular and periadnexal lymphocytic infiltration and mucin deposition in the dermis. Mucin deposition could not be shown in our case, due to the lack of facility of special stains. Linear cutaneous lupus erythematosus is usually diagnosed on the basis of clinical and histopathological findings. Direct immunofluorescence is indicated only when histopathology in not conclusive.
In our case, the lesions of linear cutaneous lupus erythematosus and that on the breast were consistent with discoid lupus erythematosus, both clinically and histopathologically. Differential diagnoses considered were linear lichen planus, linear morphea, linear psoriasis and linear verrucous epidermal nevus. This case was considered as disseminated discoid lupus erythematosus, as the lesions extended beyond the face and neck.[8] There have been only limited reports of linear discoid lupus erythematosus in adults and amongst them, most of the cases had lesions of linear cutaneous lupus erythematosus, confined to either single extremity, trunk, chest or breast.[2],[4],[9] However, we did not find any previous report of such an extensive involvement with dissemination like in the present case. In contrast to the previous reports, our patient showed remarkable therapeutic response within 6 months.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Abe M, Ishikawa O, Miyachi Y. Linear cutaneous lupus erythematosus following the lines of Blaschko. Br J Dermatol 1998;139:307-10.
[Google Scholar]
|
| 2. |
Davies MG, Newman P. Linear cutaneous lupus erythematosus in association with ipsilateral submandibular myoepithelial sialadenitis. Clin Exp Dermatol 2001;26:56-8.
[Google Scholar]
|
| 3. |
Gaitanis G, Nomikos K, Chaniotakis I, Stergiopoulou C, Zioga A, Bassukas I. Linear cutaneous lupus erythematosus: A subset of childhood cutaneous lupus erythematosus. Lupus 2009;18:759-61.
[Google Scholar]
|
| 4. |
Röckmann H, Feller G, Schadendorf D, Goerdt S. Subacute cutaneous lupus erythematosus on the lines of Blaschko. Eur J Dermatol 2006;16:302-6.
[Google Scholar]
|
| 5. |
Aiyama A, Muro Y, Sugiura K, Onouchi H, Akiyama M. Extraordinarily long linear cutaneous lupus erythematosus along the lines of Blaschko. Dermatol Online J 2013;19:18960.
[Google Scholar]
|
| 6. |
Thind CK, Husain EA, Hewitt J. A rare linear atrophic lesion on the face. Clin Exp Dermatol 2009;34:e447-8.
[Google Scholar]
|
| 7. |
Kim J, Lee SH, Roh MR. Linear cutaneous lupus erythematosus on the midline of the face. J Dermatol 2011;38:609-12.
[Google Scholar]
|
| 8. |
Goodfield MJ, Jones SK, Veale DJ. The connective tissue diseases (Discoid Lupus Erythematosus). In: Burns T, Breathnach S, Cox N, Griffiths C, editors. Rook's Textbook of Dermatology. 7th ed. Oxford: Blackwell Science Ltd.; 2004. p. 5-24.
[Google Scholar]
|
| 9. |
Heid E, Grosshans E, Gonda J, Paré M, Lipsker D. Blaschkolinear eruption with biological signs of lupus. Ann Dermatol Venereol 1996;123:331-3.
[Google Scholar]
|
Fulltext Views
3,948
PDF downloads
1,692





![[Figure - 1]](#fig_ijdvl_2017_83_5_586_210640_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2017_83_5_586_210640_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2017_83_5_586_210640_f3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2017_83_5_586_210640_f4.jpg){kind=link}
![[Figure - 5]](#fig_ijdvl_2017_83_5_586_210640_f5.jpg){kind=link}
![[Figure - 6]](#fig_ijdvl_2017_83_5_586_210640_f6.jpg){kind=link}