Translate this page into:
Disseminated Kaposi's sarcoma in a human immunodeficiency virus-infected homosexual Indian man
Correspondence Address:
Savita Yadav
Department of Dermatology and Venereology, Teaching Block, All India Institute of Medical Sciences, New Delhi
India
| How to cite this article: Bhatia R, Shubhdarshini S, Yadav S, Ramam M, Agarwal S. Disseminated Kaposi's sarcoma in a human immunodeficiency virus-infected homosexual Indian man. Indian J Dermatol Venereol Leprol 2017;83:78-83 |
Sir,
Kaposi's sarcoma has rarely been reported from India [1] though the burden of human immunodeficiency virus (HIV) infection in India is second only to that in sub-Saharan Africa, and human herpesvirus-8, the Kaposi sarcoma associated-virus is known to be prevalent here.
A 26-year-old HIV-positive male student from North India was referred to us for the evaluation of widespread violaceous plaques and nodules on the skin. The plaques had first been noticed on the dorsa of his hands 6 months back and then gradually spread to involve other parts of the body over the next few months. The patient complained of malaise and decreased appetite for the past 2 months. He had been detected to be seropositive for HIV-1 infection 3 years earlier in a voluntary screening camp but did not take antiretroviral treatment. Two months back, he was diagnosed with abdominal tuberculosis and was started on both anti-tubercular and antiretroviral treatment. There was a history of high-risk sexual behavior with multiple protected as well as unprotected homosexual exposures involving both insertive and receptive intercourse. There was no history of blood transfusion or of recreational intravenous drug use. On cutaneous examination, there were multiple (around fifty), well-defined, non-scaly, discrete, violaceous, non-tender plaques and nodules of various sizes (1–2.5 cm) scattered on the face, trunk and extremities [Figure - 1]a and [Figure - 1]b. Lesions were distributed in a 'Christmas tree-pattern' on the trunk. A similar plaque was present on the hard palate. Scalp, palms, soles and nails were normal. There was generalized lymphadenopathy: axillary, cervical and inguinal lymph nodes were enlarged (1.5–2.5 cm). They were firm, mobile, non-tender and non-matted. There was no organomegaly. Hemogram and serum biochemistry were unremarkable. Enzyme-linked immunosorbent assay (ELISA) for HIV-1 was positive and the CD4 count was 173 cells/mm [3]. Venereal disease research laboratory (VDRL), hepatitis B surface antigen and anti- hepatitis C virus antibody tests were negative. Biopsy of a plaque on the abdomen showed a spindle cell proliferation with slit-like congested capillaries dissecting between collagen bundles throughout the dermis, present individually as well as in groups with extravasation of erythrocytes. The “promontory sign” was noted [Figure - 2]a and [Figure - 2]b. The tumor cells stained positively with endothelial markers CD31 and CD34, confirming their vascular lineage. They also stained positively for human herpesvirus-8, confirming the diagnosis of Kaposi's sarcoma [Figure - 2]c. Fine needle aspiration of an inguinal lymph node showed reactive lymphoid hyperplasia. A computed tomography (CT) scan of the chest and abdomen showed flame-shaped opacities in the hilar regions bilaterally, suggesting pulmonary involvement [Figure - 3]. Endoscopy of the upper and lower gastrointestinal tracts did not show any abnormalities. With a final diagnosis of disseminated Kaposi's sarcoma (cutaneous and pulmonary involvement), the patient was treated with doxorubicin 20 mg/m [2] given as 3-weekly cycles, and antiretroviral treatment was continued. After six cycles of chemotherapy, there was significant flattening of all the skin plaques [Figure - 1]c There were no treatment-related adverse effects. Post-treatment, the CD4 count had increased to 201 cells/mm [3]. Three months after the completion of chemotherapy, there was further flattening of the plaques and nodules, along with complete resolution of the pulmonary opacities. However five months after completion of chemotherapy there was a relapse of cutaneous disease in the form of a single firm dusky erythematous nodule measuring 2 × 2 cm on the chin. Relapse was confirmed by a biopsy from the nodule which showed features of Kaposi's sarcoma. The patient is planned for 6 cycles of paclitaxel chemotherapy.
 |
| Figure 1a: Multiple violaceous and dusky erythematous plaques and nodules on the anterior trunk. The shape of many plaques is linear along the skin creases |
 |
| Figure 1b: Close-up view of the plaques and nodules on the chest |
 |
| Figure 1c: Marked flattening of plaques and nodules after completion of chemotherapy leaving behind hyperpigmentation |
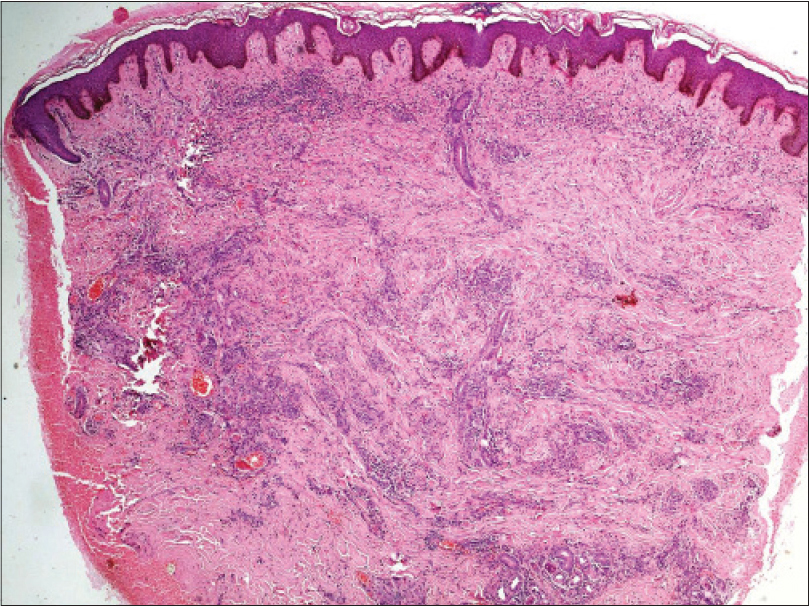 |
| Figure 2a: Dense aggregates of spindle cell proliferation in the superficial, mid- and deep dermis with congested capillaries (H and E, ×100) |
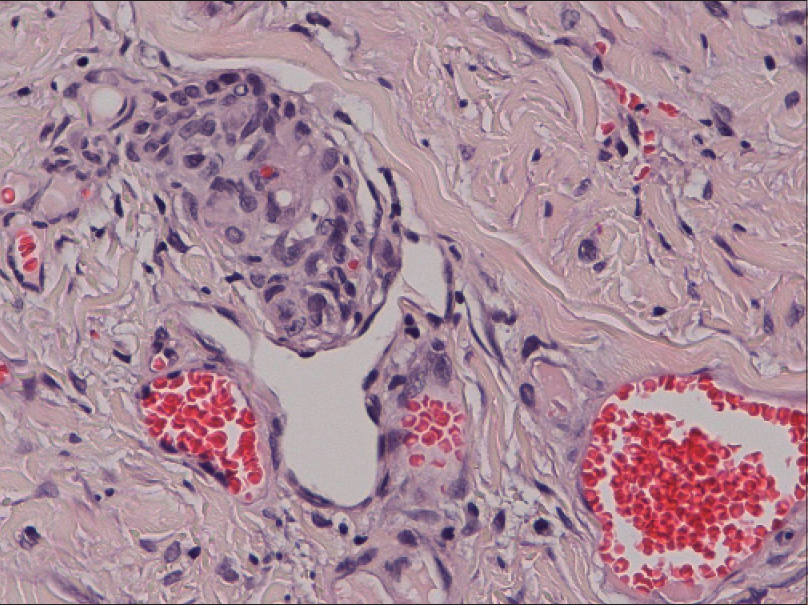 |
| Figure 2b: “Promontory sign” showing proliferation of irregular, jagged vascular channels surrounding preexisting blood vessels (H and E, ×400) |
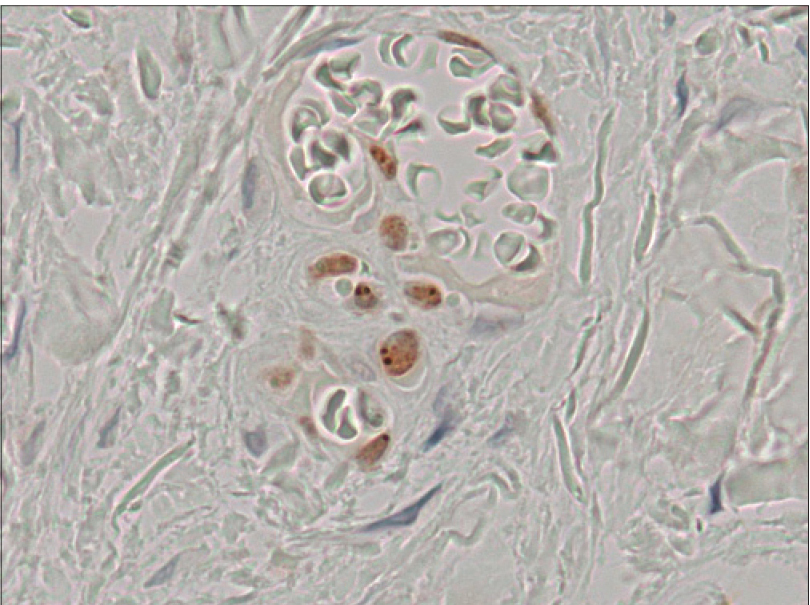 |
| Figure 2c: Positive staining of spindle cells for human herpesvirus-8 (immunohistochemical staining for latencyassociated nuclear antigen of human herpesvirus-8, ×400) |
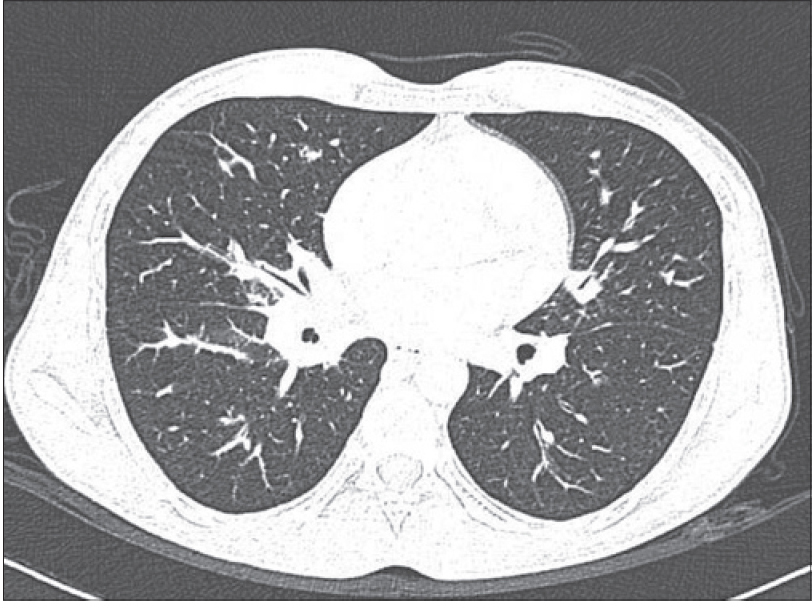 |
| Figure 3: Flame-shaped opacities in both lungs |
There are four clinical variants of Kaposi's sarcoma described: classical, African-endemic, immunosuppressive therapy-associated and acquired immune deficiency syndrome (AIDS)-associated.[2] A necessary factor implicated in the causation of Kaposi's sarcoma is human herpesvirus-8, also known as Kaposi's sarcoma-associated herpesvirus. Seroprevalence of human herpesvirus-8 varies from 50% in the general population in sub-Saharan Africa to around 6% in the United States. In India, seroprevalence was found to range from 4.7% in 379 patients (309 HIV infected and 70 healthy individuals) in South India to 26% in 165 HIV-positive, antiretroviral therapy-naïve patients in North India.[3],[4], A wide variation in human herpesvirus-8 seroprevalence has previously been observed in East Asian countries namely, Japan (11.7%), China (12.7–43.2%) and Thailand (1–28.1%).[5],[6],[7] Some studies suggest that regions high in silicaceous volcanic soil and blood-sucking insects are hot spots of human herpesvirus-8, but the exact cause for this remains unknown. It has been seen that the burden of Kaposi's sarcoma is higher in areas which are endemic for human herpesvirus-8. However, our patient had not traveled abroad to areas endemic for human herpesvirus-8 infection.
Apart from human herpesvirus-8, other factors implicated in the causation of Kaposi's sarcoma are interlekuin-6 polymorphisms and genetic variations in the human leukocyte antigen (HLA) loci, which may explain the low prevalence of Kaposi's sarcoma in India. However, we found no published genetic studies of the presence of such variations.
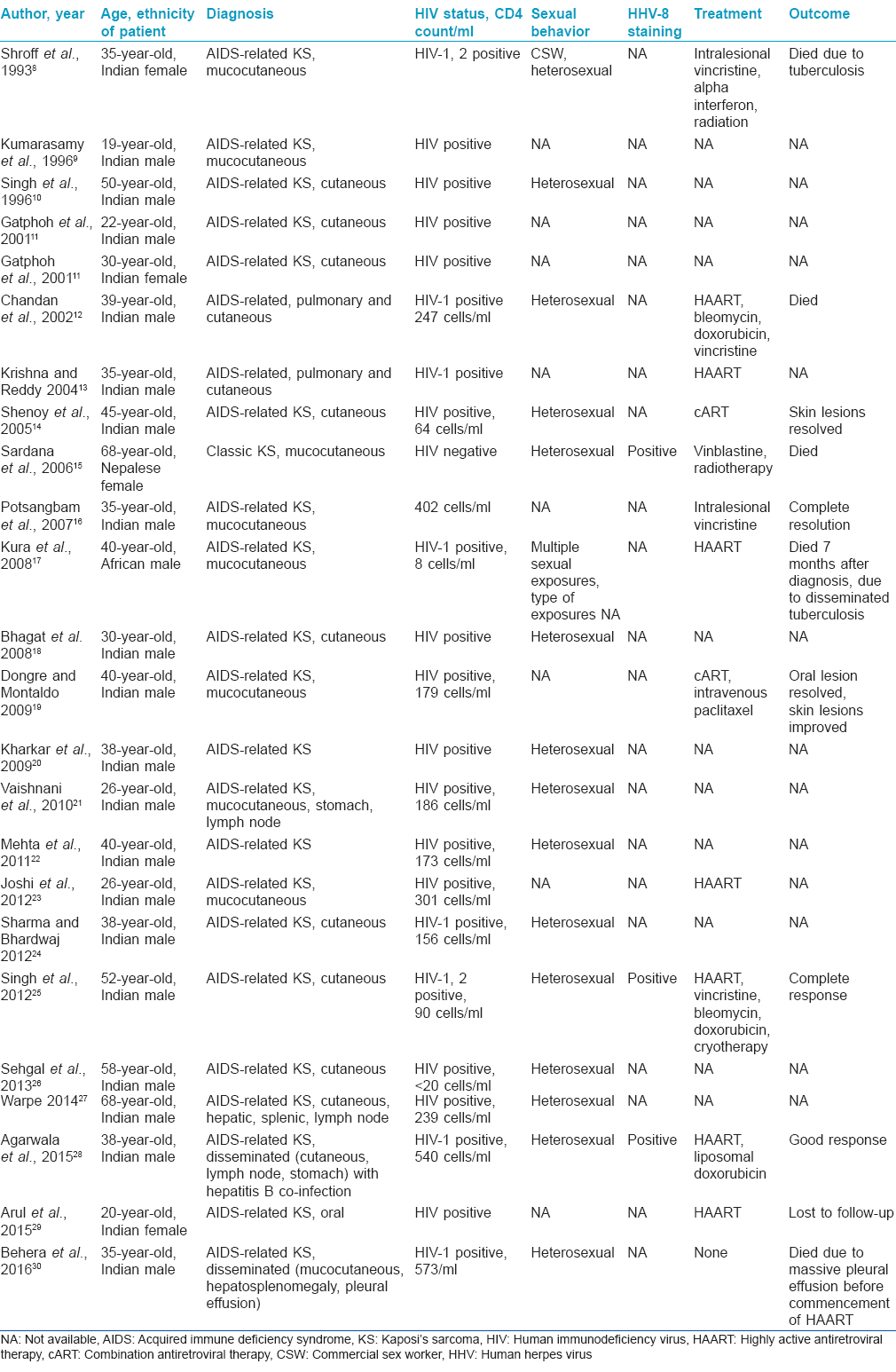
An online search was done on the PubMed database using the key words “Kaposi's sarcoma,” “cutaneous” and “India.” Relevant articles as well as those they cited were studied. Since the description of the first case of Kaposi's sarcoma in India in 1993, 23 more cases have been reported [Table - 1].[8],[9],[10],[11],[12],[13],[14],[15],[16],[17],[18],[19],[20],[21],[22],[23],[24],[25],[26],[27],[28],[29],[30] All but one were seropositive for HIV. Three cases were documented to be positive for human herpesvirus-8 infection. Elsewhere, Kaposi's sarcoma has been reported to be more common in men having sex with men (5.7 and 0.7/100 person years in men having sex with men and heterosexual men, respectively).[31] However, all the previous reports from India were of heterosexual men and women, though our patient was homosexual.
Treatment includes local modalities such as cryotherapy, intralesional vincristine and radiation therapy. Indications for systemic therapy include visceral involvement, extensive Kaposi's sarcoma associated with lymphedema, extensive and rapidly progressing Kaposi's sarcoma and failure to respond to local therapy. We administered liposomal doxorubicin, the current first-line chemotherapeutic agent for Kaposi's sarcoma because of pulmonary involvement. The risk of relapse following chemotherapy has been found to be 13.5%/year, usually occurring in the first year after treatment. In a study involving 140 patients with advanced stage Kaposi's sarcoma-AIDS treated with a combination of highly active antiretroviral therapy and liposomal anthracycline, the 5-year overall survival was found to be 85%.[32] Pulmonary Kaposi's sarcoma has a poor prognosis with a median survival of 1.6 years.[33] The 5-year survival in patients with pulmonary Kaposi's sarcoma was found to be lower than in those with classic Kaposi's sarcoma in a cohort of 305 HIV-positive patients.[34]
Acknowledgment
We are grateful to Dr. Beth Ruben, Professor of Clinical Dermatology and Pathology, University of California, San Francisco, for her help with human herpesvirus-8 immunohistochemical staining.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Available from: http://www.unaids.org/en/resources/campaigns/2014/2014gapreport/gapreport. [Last accessed on 2016 Mar 04].
[Google Scholar]
|
| 2. |
Tappero JW, Conant MA, Wolfe SF, Berger TG. Kaposi's sarcoma. Epidemiology, pathogenesis, histology, clinical spectrum, staging criteria and therapy. J Am Acad Dermatol 1993;28:371-95.
[Google Scholar]
|
| 3. |
Sachithanandham J, Kannangai R, Abraham AM, Fletcher GJ, Abraham OC, Daniel D, et al. Human herpes virus-8 infections among subjects with human immunodeficiency virus infection and normal healthy individuals in India. Intervirology 2013;56:253-7.
[Google Scholar]
|
| 4. |
Munawwar A, Sharma SK, Gupta S, Singh S. Seroprevalence and determinants of Kaposi sarcoma-associated human herpesvirus 8 in Indian HIV-infected males. AIDS Res Hum Retroviruses 2014;30:1192-6.
[Google Scholar]
|
| 5. |
Katano H, Yokomaku Y, Fukumoto H, Kanno T, Nakayama T, Shingae A, et al. Seroprevalence of Kaposi's sarcoma-associated herpesvirus among men who have sex with men in Japan. J Med Virol 2013;85:1046-52.
[Google Scholar]
|
| 6. |
Zhang T, Lin H, Minhas V, Zhu W, Wood C, He N. Prevalence and correlates of Kaposi's sarcoma-associated herpesvirus infection in a sample of men who have sex with men in Eastern China. Epidemiol Infect 2013;141:1823-30.
[Google Scholar]
|
| 7. |
Ayuthaya PI, Katano H, Inagi R, Auwanit W, Sata T, Kurata T, et al. The seroprevalence of human herpesvirus 8 infection in the Thai population. Southeast Asian J Trop Med Public Health 2002;33:297-305.
[Google Scholar]
|
| 8. |
Shroff HJ, Dashatwar DR, Deshpande RP, Waigmann HR. AIDS-associated Kaposi's sarcoma in an Indian female. J Assoc Physicians India 1993;41:241-2.
[Google Scholar]
|
| 9. |
Kumarasamy N, Solomon S, Yesudian P, Sugumar P. First report of Kaposi's sarcoma in and AIDS patient from Madras, India. Indian J Dermatol 1996;41:23-5.
[Google Scholar]
|
| 10. |
Singh RV, Singh S, Pandey SS. Numerous giant mollusca contagiosa and kaposi's sarcomas with HIV disease. Indian J Dermatol Venereol Leprol 1996;62:173-4.
[Google Scholar]
|
| 11. |
Gatphoh ED, Zamzachin G, Devi SB, Punyabati P. AIDS related malignant disease at regional institute of medical sciences. Indian J Pathol Microbiol 2001;44:1-4.
[Google Scholar]
|
| 12. |
Chandan K, Madnani N, Desai D, Deshpande R. AIDS-associated Kaposi's sarcoma in a heterosexual male – A case report. Dermatol Online J 2002;8:19.
[Google Scholar]
|
| 13. |
Krishna AG, Reddy GV. Kaposi's sarcoma in a follow-up patient of malignant schwannoma after seroconversion. Indian J Surg 2004;66:110-1.
[Google Scholar]
|
| 14. |
Shenoy VV, Joshi SR, Duberkar D, Kadam KN, Shedge RT, Lanjewar DN. Kaposi's sarcoma with thrombocytopenia in a heterosexual Asian Indian male. J Assoc Physicians India 2005;53:486-8.
[Google Scholar]
|
| 15. |
Sardana K, Mahajan S, Bhushan P, Mendiratta V. Classic Kaposi's sarcoma in a Nepalese woman from a purportedly nonendemic area. Clin Exp Dermatol 2006;31:232-4.
[Google Scholar]
|
| 16. |
Potsangbam G, Sharma SS, Singh TJ, Singh YN, Parikshit S. Intra-lesional injection of vinblastine in a pedunculated oral Kaposi's sarcoma in a patient of AIDS. J Indian Acad Clin Med 2007;8:99-100.
[Google Scholar]
|
| 17. |
Kura MM, Khemani UN, Lanjewar DN, Raghuwanshi SR, Chitale AR, Joshi SR. Kaposi's sarcoma in a patient with AIDS. J Assoc Physicians India 2008;56:262-4.
[Google Scholar]
|
| 18. |
Bhagat U, Sharma A, Marfatia YS. Violaceous papulonodular lesions in an AIDS case. Indian J Sex Transm Dis 2008;29:51-3.
[Google Scholar]
|
| 19. |
Dongre A, Montaldo C. Kaposi's sarcoma in an HIV-positive person successfully treated with paclitaxel. Indian J Dermatol Venereol Leprol 2009;75:290-2.
[Google Scholar]
|
| 20. |
Kharkar V, Gutte RM, Khopkar U, Mahajan S, Chikhalkar S. Kaposi's sarcoma: A presenting manifestation of HIV infection in an Indian. Indian J Dermatol Venereol Leprol 2009;75:391-3.
[Google Scholar]
|
| 21. |
Vaishnani JB, Bosamiya SS, Momin AM. Kaposi's sarcoma: A presenting sign of HIV. Indian J Dermatol Venereol Leprol 2010;76:215.
[Google Scholar]
|
| 22. |
Mehta S, Garg A, Gupta LK, Mittal A, Khare AK, Kuldeep CM. Kaposi's sarcoma as a presenting manifestation of HIV. Indian J Sex Transm Dis 2011;32:108-10.
[Google Scholar]
|
| 23. |
Joshi U, Ceena DE, Ongole R, Sumanth KN, Boaz K, Jeena Priy K, et al. AIDS related Kaposi's sarcoma presenting with palatal and eyelid nodule. J Assoc Physicians India 2012;60:50-3.
[Google Scholar]
|
| 24. |
Sharma RK, Bhardwaj S. Kaposi sarcoma presenting as an index sign of HIV infection in an Indian. JK Science 2012;14:158-60.
[Google Scholar]
|
| 25. |
Singh AS, Atam V, Das L. Response of ART and chemotherapy in AIDS associated Kaposi's sarcoma. J Case Rep 2012;2:125-9.
[Google Scholar]
|
| 26. |
Sehgal VN, Verma P, Sharma S. HIV/AIDS Kaposi sarcoma: The Indian perspective. Skinmed 2013;11:375-7.
[Google Scholar]
|
| 27. |
Warpe BM. Kaposi sarcoma as initial presentation of HIV infection. N Am J Med Sci 2014;6:650-2.
[Google Scholar]
|
| 28. |
Agarwala MK, George R, Sudarsanam TD, Chacko RT, Thomas M, Nair S. Clinical course of disseminated Kaposi sarcoma in a HIV and hepatitis B co-infected heterosexual male. Indian Dermatol Online J 2015;6:280-3.
[Google Scholar]
|
| 29. |
Arul AS, Kumar AR, Verma S, Arul AS. Oral Kaposi's sarcoma: Sole presentation in HIV seropositive patient. J Nat Sci Biol Med 2015;6:459-61.
[Google Scholar]
|
| 30. |
Behera B, Chandrashekar L, Thappa DM, Toi PC, Vinod KV. Disseminated Kaposi's sarcoma in an HIV-positive patient: A rare entity in an Indian patient. Indian J Dermatol 2016;61:348.
[Google Scholar]
|
| 31. |
Atkinson JO, Biggar RJ, Goedert JJ, Engels EA. The incidence of Kaposi sarcoma among injection drug users with AIDS in the United States. J Acquir Immune Defic Syndr 2004;37:1282-7.
[Google Scholar]
|
| 32. |
Bower M, Dalla Pria A, Coyle C, Andrews E, Tittle V, Dhoot S, et al. Prospective stage-stratified approach to AIDS-related Kaposi's sarcoma. J Clin Oncol 2014;32:409-14.
[Google Scholar]
|
| 33. |
Biggar RJ, Engels EA, Ly S, Kahn A, Schymura MJ, Sackoff J, et al. Survival after cancer diagnosis in persons with AIDS. J Acquir Immune Defic Syndr 2005;39:293-9.
[Google Scholar]
|
| 34. |
Palmieri C, Dhillon T, Thirlwell C, Newsom-Davis T, Young AM, Nelson M, et al. Pulmonary Kaposi sarcoma in the era of highly active antiretroviral therapy. HIV Med 2006;7:291-3.
[Google Scholar]
|
Fulltext Views
8,198
PDF downloads
2,520





![[Figure - 1]](#fig_ijdvl_2017_83_1_78_193612_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2017_83_1_78_193612_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2017_83_1_78_193612_f3.jpg){kind=link}
![[Table - 1]](#tbl_ijdvl_2017_83_1_78_193612_t8.jpg){kind=link}