Translate this page into:
Eruptive pruritic papular porokeratosis
Correspondence Address:
Shang-Ian Tee
National Skin Centre, 1 Mandalay Road, Singapore 308 205
Singapore
| How to cite this article: Tee SI, Chong WS. Eruptive pruritic papular porokeratosis. Indian J Dermatol Venereol Leprol 2012;78:758-760 |
Sir,
A 63-year-old Chinese man was referred for a papulosquamous eruption affecting his buttocks, groin, and forearms, which had been recurring over the past 13 years. He gave the history of repeated acute episodes of intense pruritus accompanied by the appearance of new lesions. Previous treatment consisted only of topical corticosteroids prescribed by his family physician. With therapy, his itch resolved and the skin lesions subsided with hyperpigmentation. There were no known triggers for the exacerbations, he was not known to suffer from any chronic illnesses, and he was not on any concurrent medications.
Physical examination of the buttocks revealed multiple erythematous scaly annular plaques with ridged edges forming collarettes of scales, interspersed with older annular hyperpigmented macules [Figure - 1]. Similar clinical findings were also noted on examination of his forearms.
 |
| Figure 1: Multiple annular scaly papulosquamous plaques and hyperpigmented macules (buttocks) |
A skin biopsy specimen was taken from a lesion on his right gluteal cleft. There was compact hyperkeratosis with oblique parakeratotic tiers (i.e. cornoid lamellae) arising within keratin-filled invaginations [Figure - 2]a. Intracorneal neutrophils or fungal elements were not present. There was an irregular epidermal hyperplasia with an absent granular layer and dyskeratotic cells. A superficial perivascular lymphocytic infiltrate was seen in the upper dermis [Figure - 2]b.
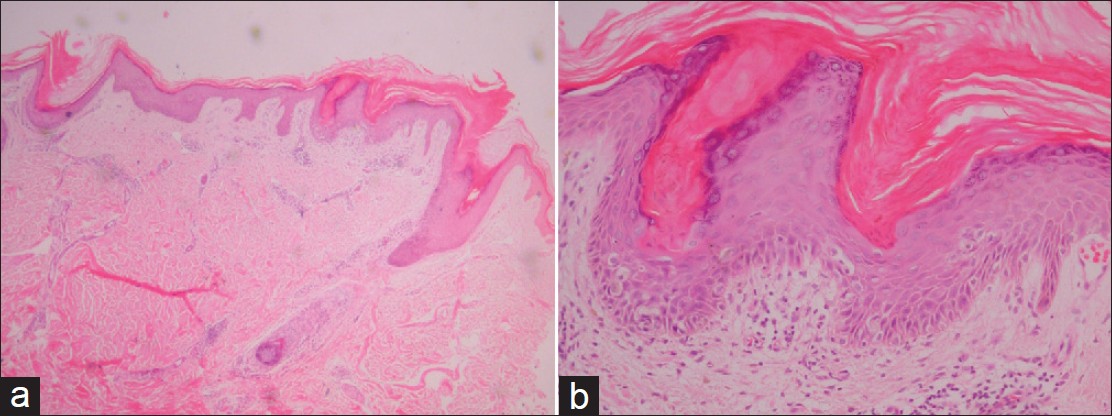 |
| Figure 2: (a) Skin biopsy showed compact hyperkeratosis with oblique parakeratotic tiers (H and E, × 20), (b) Skin biopsy showed epidermal hyperplasia, absent granular layer and dyskeratotic cells (H and E, ×100) |
The histology report was consistent with porokeratosis. Together with the clinical picture of a chronic persistent rash marked by recurrent acute pruritic exacerbations, the diagnosis of eruptive pruritic papular porokeratosis (EPPP) was made.
EPPP was first described by Kanzaki et al as a variant of disseminated superficial porokeratosis (DSP). [1] The latter is classically an asymptomatic dermatosis. [2] EPPP differs from DSP in this respect, as it clinically presents with repeated flares of intense pruritus together with the appearance of new lesions, as with our patient. Histological features are identical in both conditions. In a review of 8 previously reported cases, [3] 7 out of 8 had pre-existing lesions lasting at least a year. Regression within 12 months was observed in 6 out of the 8 cases.
EPPP had been reported in a patient with colon cancer. [4] This patient was diagnosed with cancer 6 years prior and underwent surgical resection followed by adjuvant chemotherapy. His cutaneous lesions appeared 3 years later and were initially asymptomatic, with acute pruritic lesions developing subsequently. An abnormal p53 tumor suppressor gene expression had been suggested as a possible common pathway for development of DSP and carcinogenesis, although a causal link was not conclusively established. Our patient did not have a personal history of cancer, and he defaulted follow-up before cancer screening could be instituted.
EPPP is a rare variant of porokeratosis with only around 10 cases previously reported in the English literature. [4] Its peculiar relapsing, pruritic presentation sets this condition apart from other forms of porokeratosis. Although the lesions of EPPP tend to resolve over a period of months, topical and/or systemic treatment may be indicated for severe pruritus. In our patient, only topical steroids and oral antihistamines were prescribed, resulting in partial improvement of symptoms. Etretinate was used in a patient resulting in remission after one year. [5] In general, however, response to therapy is variable.
| 1. |
Kanzaki T, Miwa N, Kobayashi T, Ogawa S. Eruptive pruritic papular porokeratosis. J Dermatol 1992;19:109-12.
[Google Scholar]
|
| 2. |
Cockerell CJ, Larsen F. Benign Epidermal Tumors and Proliferations. In: Bolognia JL, editor. Dermatology, 2 nd ed. St. Louis: Mosby; 2007. p. 1661-80.
[Google Scholar]
|
| 3. |
Kanekura T, Yoshii N. Eruptive pruritic papular porokeratosis: A pruritic variant of porokeratosis. J Dermatol 2006;33:813-6.
[Google Scholar]
|
| 4. |
Choi KH, Kim TY. A case of inflammatory disseminated superficial porokeratosis in a colon cancer patient. Ann Dermatol 2009;21:150-3.
[Google Scholar]
|
| 5. |
Stork J, Kodetová D. Disseminated superficial porokeratosis: An eruptive pruritic papular variant. Dermatol 1997;195:304- 5.
[Google Scholar]
|
Fulltext Views
2,086
PDF downloads
1,111





![[Figure - 1]](#fig_ijdvl_2012_78_6_758_102384_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2012_78_6_758_102384_f2.jpg){kind=link}