Translate this page into:
Erythema gyratum repens and rheumatoid arthritis: An unrecognized association?
2 Department of Rheumatology, Second University of Naples, Via Pansini 5, 80131 Naples, Italy
Correspondence Address:
Stefano Caccavale
Via Pansini 5, 80131, Naples
Italy
| How to cite this article: Lo Schiavo A, Caccavale S, Orlando I, Tirri R. Erythema gyratum repens and rheumatoid arthritis: An unrecognized association?. Indian J Dermatol Venereol Leprol 2012;78:122 |
Sir,
A 62-year-old Caucasian man was referred to us with multiple erythematous arciform lesions with a wood-grain-like appearance of fifteen months′ evolution. The dermatosis had initially affected the patient′s legs, extending to his abdomen and arms. His medical history included rheumatoid arthritis, treated with systemic corticosteroids; DMARDs (methotrexate) with folic acid supplements; omeprazole; and cardioaspirin. Interestingly, the resolution of rheumatoid arthritis with various DMARDs was related to the resolution of the dermatosis. Physical examination disclosed an eruption on the legs characterized by irregular, multiple, gyrate bands of erythema bordered on one side by scale and on the other by normal-looking skin. The lesions migrated, leaving a thin scale at the edges and creating a bizarre pattern [Figure - 1]. The dermatosis exhibited characteristic rapid movement over hours. Pruritus was moderate. The patient had previously taken oral corticosteroids which had been partially successful, but his condition had worsened rapidly when treatment was interrupted.
Histopathological findings were non-specific, showing evidence of hyperkeratosis, orthokeratosis, and a superficial, perivascular, mononuclear infiltrate, which although non-diagnostic, were consistent with changes described for erythema gyratum repens (EGR) [Figure - 2]. Several case reports have shown positive direct immunofluorescence (DIF) in the skin: DIF tests on the skin describe deposits of IgG and C3 along the basement membrane zone. [1] However, DIF of involved non-sun-exposed and uninvolved skin was negative in our patient.
 |
| Figure 1: Clinical presentation on admission |
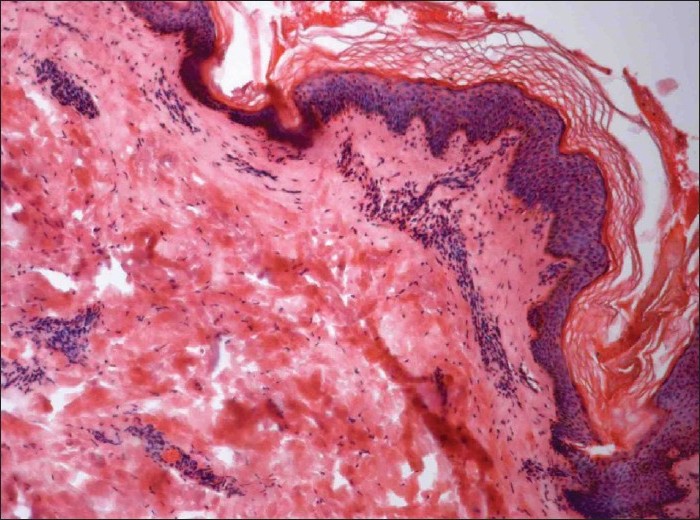 |
| Figure 2: Histological features of erythema gyratum repens (EGR) included hyperkeratosis, orthokeratosis, and a perivascular inflammatory infiltrate (H and E, ×200) |
Clinical findings were consistent with EGR. The patient had a family history of esophageal cancer, so the search for an associated neoplasm began. Laboratory tumor markers were all normal. Thirty-two months after the onset of EGR, investigations (chest X-ray, gastroscopy, colonoscopy, abdominal ultrasound, computerized tomography of the chest, abdomen and pelvis, and whole body PET-CT) still proved normal.
The presentation of the skin disorder was so distinctive that a differential diagnosis was difficult to generate. In our patient, the differential diagnoses included erythema annulare centrifugum (EAC), urticarial vasculitis, and systemic lupus erythematosus. Distinction between EGR and EAC is very difficult, since clinical findings are similar; the histopathologic pictures of both diseases are nonspecific and both can be associated with malignancy (EGR more often). However, one of the differences between them is in the rapidity of movement. EGR exhibits characteristic rapid movement over minutes and hours; EAC moves slowly over days and months. The gyrate erythema presented in this case had clinical features similar to both EGR and EAC, but the rapidity of movement was more consistent with EGR. The differential diagnosis between EGR and urticarial vasculitis was made histopathologically. Urticarial vasculitis typically shows leukocytoclastic vasculitis. Classic symptoms of urticarial vasculitis, such as painful burning sensation, residual purpura, and pigmentation, were not present. Scaling trailing the leading edge of the eruption, which is one of the typical findings of EGR, was present in our case. The patient was studied for tuberculosis; chest X-ray, CT, Mantoux test, and Quantiferon test were all negative.
EGR is a rare specific dermatosis, believed to be an obligate paraneoplastic cutaneous syndrome. In more than 80% of cases, EGR is associated with an underlying malignancy and in 80% of cases, this distinctive migratory eruption appears prior to a malignancy diagnosis. EGR can precede 1 to 72 months before malignancy, though the average is 4 to 9 months. Approximately, one-third of patients will manifest lung cancer, 8% esophageal cancer, and 6% an unknown primary. Tumors of the breast, bladder, prostate, cervix, and uterus have also been reported. [2]
Here, however, we report a case of EGR which is non-paraneoplastic. Case reports demonstrating an association with non-neoplastic diseases have also been reported, such as pulmonary tuberculosis, drug use, hypereosinophilic syndrome, ichthyosis, autoimmune conditions such as CREST syndrome [3] or disorders with an EGR-like presentation such as tinea imbricata, lupus erythematosus, bullous diseases, resolving pityriasis rubra pilaris, [4] psoriasis, and Sjφgren syndrome. [5] This association may either be an example of an extremely unusual clinical presentation of the primary dermatosis in question, or may be a case of "true" EGR as observed during the course of other non-neoplastic conditions. Healthy patients with this distinctive eruption have been reported in literature, which might cast doubt on the reliability of the diagnosis.
To our knowledge, no case of EGR associated with rheumatoid arthritis has, to date, been described in literature, making our case the first reported description of its kind. Moreover, a parallel evolution of the two affections (EGR and rheumatoid arthritis) was observed in our patient. In conclusion, our experience shows that EGR does not necessarily indicate underlying malignancy, but it can be associated with a non-neoplastic disease such as rheumatoid arthritis.
| 1. |
Caux F, Lebbe C, Thomine E, Benyahia B, Flageul B, Joly P, et al. Erythema gyratum repens: A case studied with immunofluorescence, immunoelectronmicroscopy and immunohistochemistry. Br J Dermatol 1994;131:102-7.
[Google Scholar]
|
| 2. |
Hauschild A, Swensson O, Christophers E. Paraneoplastic bullous pemphigoid resembling erythema gyratum repens. Br J Dermatol 1999;140:550-2.
[Google Scholar]
|
| 3. |
Demonchy E, Lacour JP, Ortonne JP, Passeron T. Erythema gyratum repens, not always a bad omen for patients. J Eur Acad Dermatol Venereol 2010;24:738-9.
[Google Scholar]
|
| 4. |
Almaani N, Robson A, Sarkany R, Griffiths WA. Erythema gyratum repens associated with pityriasis rubra pilaris. Clin Exp Dermatol 2011;36:161-4.
[Google Scholar]
|
| 5. |
Matsumura T, Kumakiri M, Sato-Matsumura KC, Ohkawara A. Erythema gyratum repens-like eruption in a patient with Sjögren syndrome. Acta Derm Venereol 1995;75:327.
[Google Scholar]
|
Fulltext Views
3,708
PDF downloads
3,601





![[Figure - 1]](#fig_ijdvl_2012_78_1_122_90974_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2012_78_1_122_90974_f2.jpg){kind=link}