Translate this page into:
Erythematous indurated plaque lesions on the breast
2 Department of Pathology, Mustafa Kemal University School of Medicine, Hatay, Turkey
3 Department of General Surgery, Mustafa Kemal University School of Medicine, Hatay, Turkey
Correspondence Address:
Bilge B�lb�l Sen
Department of Dermatology, Mustafa Kemal University, Tayfur Ata Sokmen Medical School, Serinyol, Antakya, Hatay 31005
Turkey
| How to cite this article: Sen BB, Rifaioğlu EN, Ekiz �, �zg�r T, Akk���k S, İnan MU, Doğramacı A�. Erythematous indurated plaque lesions on the breast. Indian J Dermatol Venereol Leprol 2013;79:849 |
A 50-year-old female patient, who had retraction of the right nipple for 2 years and erythema in the same breast for 2 months, was referred to our clinic. Mammography and breast ultrasonography performed at the time of onset of nipple retraction were normal. Dermatological examination revealed three erythematous, mildly indurated plaque lesions on the right breast, one of which involved the areola [Figure - 1]. The nipple was retracted. The patient had no subjective complaints. The right axillary examination detected several lymphadenopathies, as confirmed by ultrasonography. The histopathological examination of the skin biopsy revealed islands of tumor cells in the dermal lymphatics [Figure - 2]. These infiltrations consisted of round-shaped atypical cells with vesiculated nuclei and marked nucleoli. In immunohistochemical studies, strong positive staining by low-molecular weight keratin (LMWCK) and epithelial membrane antigen (EMA) and non-specific staining by vimentin have been detected.
 |
| Figure 1: Three erythemateous plaques on the right breast, one involving the areola |
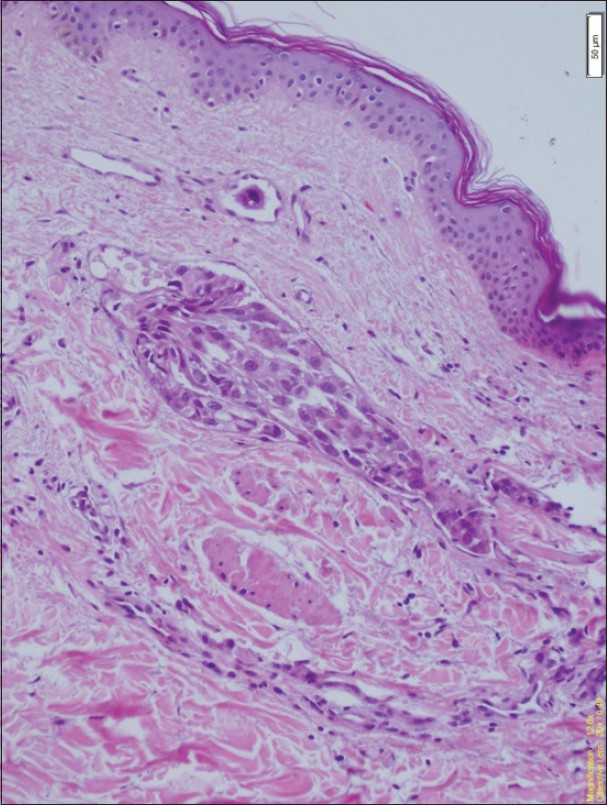 |
| Figure 2: Tumor islands consisted of atypical epithelium cells in the lymphatics (H and E, ×200) |
What is your Diagnosis?

Discussion
The rate of skin metastasis in internal malignancies varies from 0.7 to 10%. [1] The skin metastases may occur as a result of lymphogenous, hematogenous spread, or direct invasion of surrounding tissue by tumor cells. Skin metastases usually occur as a finding of the spread or the recurrence of internal malignancies; however, they may rarely be an initial finding of an undetected malignancy.
Carcinoma erysipeloides (CE) is a rare cutaneous metastasis, which results from the lymphatic spread of an inflammatory carcinoma. While it is mostly related to breast cancer, it may also result from other tumors. [2],[3],[4] In our case, a solid mass lesion was also detected in the right breast, and the biopsy performed at the General Surgery Department was reported as invasive ductal carcinoma.
In the differential diagnosis of CE, erysipelas, cellulitis, radiation dermatitis, and contact dermatitis should be considered. The exact diagnosis of CE is made by histopathology. The dermal lymphatic invasion is considered as the characteristic feature of CE.
Other than breast cancer, nipple retraction may occur due to periductal mastitis, ductal ectasia, tuberculosis, sarcoidosis, fungal infections, and granulomatous inflammatory diseases, including Wegener′s granulomatosis and idiopathic granulomatosis lobular mastitis. [5] In our case, nipple retraction began 2 years ago, and the laboratory examinations performed at that time revealed no pathology. Therefore, nipple retraction was not considered to be associated with breast cancer.
In general, CE develops several months or years after the diagnosis of primary carcinoma. CE is an indicator of poor prognosis, and patients often die within few months of its diagnosis. CE developing as an initial sign of undiagnosed tumor is rare. [2] Interestingly, in our patient, CE was diagnosed before the diagnosis of breast cancer.
In cases of CE, treatment of primary tumor is sufficient. Surgical treatment is not recommended. Systemic chemotherapy and hormonal therapies alone or in combination with radiotherapy represent the basic treatment options. [2] We also referred our patient to the general surgery and oncology departments for planning the treatment of primary tumor.
Conclusion
While the skin metastases generally occur after the diagnosis of primary tumor, they may also develop prior to diagnosis. The skin invasions can be clinically confused with other disorders. This may result in delayed diagnosis of the malignancy and decrease in survival. Our case demonstrated the importance of non-specific skin lesions such as erythema in diagnosis of breast cancer. Therefore, the dermatologists should be careful with respect to cutaneous metastases, even if the patient′s medical history does not include malignancy.
| 1. |
Krathen RA, Orengo IF, Rosen T. Cutaneous metastasis: A meta-analysis of data. South Med J 2003;96:164-7.
[Google Scholar]
|
| 2. |
Cox SE, Cruz PD Jr. A spectrum of inflammatory metastasis to skin via lymphatics: Three cases of carcinoma erysipeloides. J Am Acad Dermatol 1994;30:304-7.
[Google Scholar]
|
| 3. |
Lee SY, Chang SE, Bae GY, Choi JH, Sung KJ, Moon KC, et al. Carcinoma erysipeloides associated with anaplastic thyroid carcinoma. Clin Exp Dermatol 2001;26:671-3.
[Google Scholar]
|
| 4. |
Nikolaou V, Stratigos A, Frangia K, Nikolaidis I, Syrigos K. Carcinoma erysipeloides deriving from a primary cutaneous squamous cell carcinoma. Int J Dermatol 2011;50:754-6.
[Google Scholar]
|
| 5. |
Nicholson BT, Harvey JA, Cohen MA. Nipple-areolar complex: Normal anatomy and benign and malignant processes. Radiographics 2009;29:509-23.
[Google Scholar]
|
Fulltext Views
6,027
PDF downloads
3,128





![[Figure - 1]](#fig_ijdvl_2013_79_6_849_120761_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2013_79_6_849_120761_f2.jpg){kind=link}