
Translate this page into:
Extensive annular petechial eruption in an elderly man with Parkinson’s disease: A clinicopathological challenge
Corresponding author: Dr. Woo Chiao Tay, Department of Dermatology, Changi General Hospital, Singapore. woochiao.tay@mohh.com.sg
-
Received: ,
Accepted: ,
How to cite this article: Tay WC, Tan SH, Lee SX. Extensive annular petechial eruption in an elderly man with Parkinson’s disease: A clinicopathological challenge. Indian J Dermatol Venereol Leprol. 2024;90:566. doi: 10.25259/IJDVL_832_2023
Case Presentation
A man in his sixties presented with a mildly pruritic, annular-looking petechial rash that first appeared on his lower limbs 2 years ago. The rash progressed upwards to his anterior trunk and cheeks. He had Parkinson’s disease and was started on co-formulated levodopa and benserazide, a few months before the rash appeared. He had no systemic symptoms, anorexia, or weight loss. His other medications include ropinirole and selegiline, both of which were started a year before rash onset.
Examination revealed extensive annular-looking petechial macules involving the lateral cheeks, neck, trunk, and both upper and lower limbs [Figures 1a and 1b]. His back and buttocks were spared. Punch biopsies of the macules on both the patient’s neck and abdomen showed superficial perivascular lymphohistiocytic infiltrates admixed with plasma cells, scattered eosinophils, and extravasated red blood cells [Figure 1c]. A few haemosiderin pigments were also identified on Perl’s stain. No dysplasia or epidermotropism of lymphocytes was seen.

- Annular petechial macules involving the anterior trunk.

- Close-up photograph of the neck and left lateral cheek, showing lesions of similar morphology.
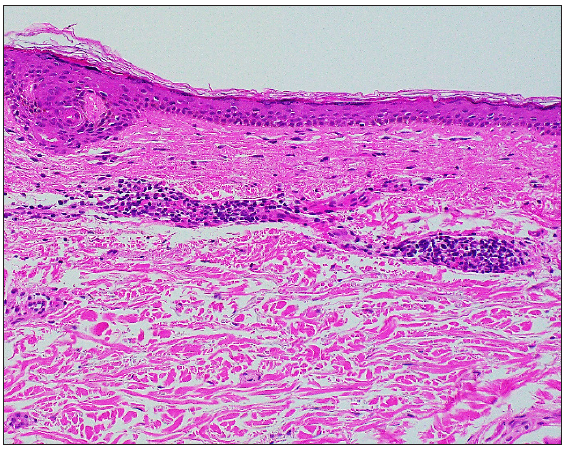
- Histology from the macules demonstrating superficial perivascular lymphohistiocytic infiltrates with plasma cells, scattered eosinophils, and extravasated red blood cells (Haematoxylin & Eosin, 200×).
Question
What is your diagnosis?
Answer
Diagnosis: Purpura annularis telangiectoides of Majocchi
Discussion
Purpura annularis telangiectodes of Majocchi (PATM), also known as Majocchi’s disease, is a subtype of pigmented purpuric dermatoses (PPD), a group of histopathologically similar capillaritis that differs by their clinical morphology. Our case illustrates a patient with an annular-looking petechial eruption but with atypical features of extensive involvement of the trunk and face after the initiation of co-formulated levodopa and benserazide. Given the temporal relationship and the presence of eosinophils, a drug reaction could be a possibility. This patient had a platelet count of 294 × 109/L.
PATM, first described in 1896, is an uncommon condition that tends to affect children and young females.1 It presents as bluish-to-red macules with dark-red telangiectatic spots and the centrifugal extension of these macules gives it its characteristic annular configuration. Dermoscopy shows irregular round-to-oval red dots, globules, and structureless areas with diffuse ill-defined brownish-red homogenous areas [Figure 1d]. Like most PPDs, PATM predominantly involves the lower limbs with extension to the upper extremities symmetrically, although an atypical unilateral presentation of PATM has been reported.2 Extensive involvement including the trunk and face, as in this case, has not been reported.
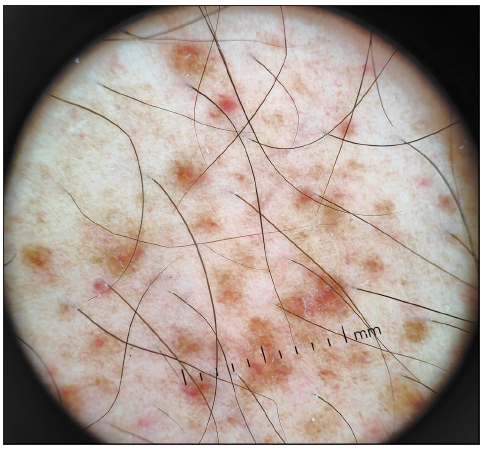
- Dermoscopy showing irregular round-to-oval red dots, globules, and structureless areas with ill-defined brownish-red homogenous areas.
PATM shares similar histopathology features with the other PPD subtypes: dilated blood vessels, erythrocyte extravasation, haemosiderin deposition, and perivascular lymphohistiocystic infiltration. In a retrospective review by Huang et al., all inflammatory reaction patterns (lichenoid, perivascular, interface, spongiotic, granulomatous) can be seen in PPD but only lichenoid and perivascular patterns were found in PATM.3
The pathogenesis of PATM and other PPD remains unknown, although venous hypertension, gravity, capillary fragility, and focal infections have been proposed as contributing factors. Drug associations with analgesics, oral hypoglycaemic agents, and anti-hypertensive agents have been reported, in particular with Schamberg disease.4 While neuroactive agents (e.g. carbromal, chlordiazepoxide, lorazepam, meprobamate) have been reported, drugs used for Parkinson’s disease, as in this case, have not been previously associated.
PATM should be differentiated from other causes of petechiae such as leukocytoclastic vasculitis with annular morphology, idiopathic thrombocytopenic purpura, PPD-like mycosis fungoides, and purpuric pityriasis rosea [Table 1]. There are also reports that PPD may mimic or progress to cutaneous T-cell lymphoma (CTCL).1,5 In 56 patients with persistent PPD, Toro et al. found 29 patients (52%) with histological features of CTCL.5 Hence, histological diagnosis should always be pursued in patients with atypical or persistent presentations of PPD.
| Feature | Purpura annularis telangiectodes of Majocchi | Idiopathic thrombocytopenic purpura | Leukocytoclastic vasculitis with annular morphology | PPD-like mycosis fungoides | Pityriasis Rosea |
|---|---|---|---|---|---|
| Age | 5th decade | 3rd to 4th decade | All ages | After 50 years of age | 2nd to 3rd decade |
| Gender predilection | Male | Female | None | Male | None |
| Location | Lower limbs | Lower limbs | Lower limbs | Lower limbs (but usually more widespread) |
Trunk with a herald patch Proximal limbs (Langer’s lines) |
| Pruritus | None to mild | None to mild | None to mild | Yes | Yes |
| Palpable lesions | No | No | Yes | No | Yes (Papulosquamous) |
| Other bleeding manifestations | No | Yes (other mucocutaneous sites) | No | No | No |
| Associations | Venous insufficiency, exercise, RA, SLE, CLL, hyperlipidaemia, drugs (NSAID, statins, CCB, ACEi, beta-blockers) | Infections (HIV, hepatitis C, CMV, VZV), drugs, SLE, APS, HIV, CVID | Infections (Streptococcus pyogenes, bacterial endocarditis, HIV, hepatitis, tuberculosis), malignancy (paraneoplastic), drugs (antibiotics, thiazides, phenytoin, allopurinol, warfarin, NSAID), autoimmune (SLE, dermatomyositis, RA) | Progression from PPD | Infections (HHV-6, HHV-7), medications (vaccines, gold, captopril, barbiturates, penicillamine, clonidine) |
| Histology | Small vessel perivascular lymphohistiocytic inflammation with endothelial cell swelling, no leukocytoclasis, extravasated red blood cells (RBC) with variable haemosiderin deposition in macrophages | Erythrocyte extravasation in the absence of vascular inflammation | Perivascular neutrophils with fibrinoid necrosis, some extravasated RBC, leukocytoclasis | Epidermotropism with infiltration by atypical lymphocytes | Subacute spongiotic dermatitis with perivascular lymphocytic infiltrates, focal extravasation of RBC without leukocytoclasis |
Legend: ACEi: Angiotensin-converting enzyme inhibitors, APS: Antiphospholipid syndrome, CCB: Calcium channel blockers, CLL: Chronic lymphocytic leukaemia, CMV: Cytomegalovirus, CVID: Common variable immunodeficiency disorders, HHV: Human herpesvirus, HIV: Human immunodeficiency virus, NSAID: Non-steroidal anti-inflammatory drugs, PPD: Pigmented purpuric dermatosis, RA: Rheumatoid arthritis, RBC: Red blood cells, SLE: Systemic lupus erythematosus, VZV: Varicella zoster virus
While PATM is a benign condition, the absence of guidelines and the persistent nature of this condition make management challenging. Conservative or non-pharmacological management (leg elevation, compression stockings) can be considered for asymptomatic patients.1 Suspected culprit drugs should be stopped where feasible. For symptomatic patients with PPD, treatment options include topical agents, such as corticosteroids and calcineurin inhibitors. Other treatment options have been described with variable success, including intralesional triamcinolone, oral agents (rutoside, ascorbic acid, pentoxifylline, venoactive agents, e.g., diosmin, calcium dobesilate, colchicine, griseofulvin, cyclosporine, methotrexate), phototherapy (narrow-band ultraviolet B phototherapy, psoralen plus ultraviolet A photochemotherapy) and laser therapy.1,4
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
References
- Purpura annularis telangiectodes of Majocchi: Case report and review of the literature. Int J Dermatol. 2009;48:1129-33.
- [CrossRef] [PubMed] [Google Scholar]
- Unilateral purpura annularis telangiectodes of majocchi in an elderly male: An atypical presentation. Dermatol Online J. 2013;19
- [PubMed] [Google Scholar]
- The pathological spectrum and clinical correlation of pigmented purpuric dermatosis—A retrospective review of 107 cases. J Cutan Pathol. 2018;45:325-32.
- [CrossRef] [PubMed] [Google Scholar]
- Pigmented purpuric dermatoses: A complete narrative review. J Clin Med. 2021;10:2283.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Persistent pigmented purpuric dermatitis and mycosis fungoides: Simulant, precursor, or both? Am J Dermatopathol. 1997;19:108-18.
- [CrossRef] [PubMed] [Google Scholar]




