Translate this page into:
Extensive inflammatory skin metastasis from ovarian carcinoma: Carcinoma erysipeloides
2 Department of Obstetrics and Gynecology, SMS Medical College, Jaipur, Rajasthan, India
3 Department of Pathology, SMS Medical College, Jaipur, Rajasthan, India
Correspondence Address:
Sunil K Kothiwala
Department of Dermatology and Venereology, SMS Medical College and Attached Hospitals, Jaipur, Rajasthan
India
| How to cite this article: Kothiwala SK, Meena M, Maheshwari A, Jindal A. Extensive inflammatory skin metastasis from ovarian carcinoma: Carcinoma erysipeloides. Indian J Dermatol Venereol Leprol 2015;81:425-427 |
Sir,
We report a patient of advanced ovarian carcinoma with the unusual manifestation of widespread cutaneous metastases in the form of multiple erythematous macules and nodules.
A 50-year-old woman who had ovarian serous cystadenocarcinoma with widespread internal metastases, presented to us with a 3-week history of erythematous macules and painful nodules over her trunk associated with fever, dyspnea and abdominal pain. Skin lesions had first appeared on the abdomen and gradually involved both the breasts. At presentation, she had multiple well- to ill-defined erythematous macules of variable size over the abdomen and chest extending up to the lateral aspect of the breasts with skip areas in between [Figure - 1]. There were multiple, erythematous to dusky red, firm, tender, papules and nodules of variable sizes which were more concentrated around her umbilicus at the site of previous surgery and on the right side of her chest and abdomen. There were a few translucent tiny vesicles on the flank. There was a firm nodule of size 3 × 2 cm in the right breast. She also had significant supraclavicular, axillary and inguinal lymphadenopathy.
 |
| Figure 1: Extensive erythematous macules with multiple papules and nodules over chest, breast, and abdomen |
She had undergone hysterectomy 4 years earlier for abnormal uterine bleeding and 6 months later, developed abdominal pain and distension. At that time, ultrasonography showed a complex multilocular cystic pelvic mass with moderate ascites and CA-125 was raised (194.2 U/ml). She underwent bilateral salpingo-oophorectomy and a final diagnosis of serous cystadenocarcinoma of the left ovary, stage Ic was made. With 6 cycles of paclitaxel and cisplatin, her CA-125 level decreased to 17.4 U/ml. Six months following her last cycle, her CA-125 level again rose to 73.4 U/ml and computed tomography (CT) of the chest showed calcified metastatic lesions in the upper and lower lobes of the right lung with mild right pleural effusion. Computed tomography of the abdomen showed multiple heterogeneously enhancing soft tissue density mass lesions in the peritoneum, focal urinary bladder wall thickening and involvement of the liver, spleen and kidney. In view of these findings, the patient was again started on the same regimen of chemotherapy.
In view of her ovarian carcinoma, the possibility of nodular cutaneous metastases with carcinoma erysipeloides was considered for her skin lesions and a punch biopsy was taken from a firm papule as well as an erythematous macule. Histopathology of the papule showed sheets and small clusters of malignant epithelial cells, with glandular pattern at places in the dermis, suggestive of adenocarcinoma of ovary [Figure - 2]a and b. The erythematous macule showed clusters of malignant cells within dilated dermal lymphatics [Figure - 3]a and b consistent with carcinoma erysipeloides. Fine-needle aspiration cytology (FNAC) of the right breast nodule and supraclavicular lymph node showed clusters of atypical cells consistent with epithelial malignancy.
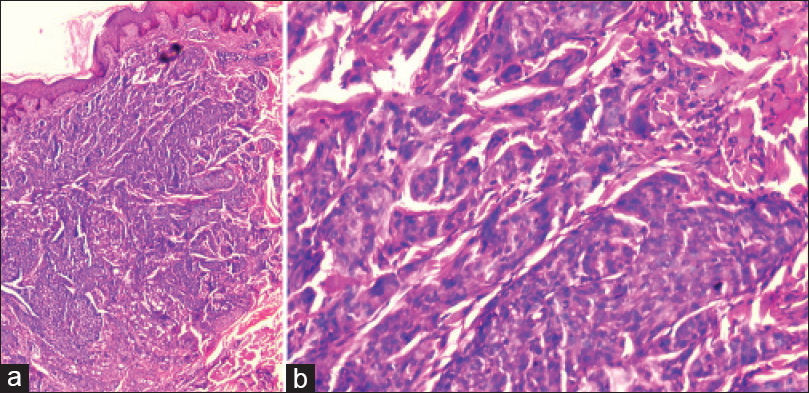 |
| Figure 2: (a) Sheets and small clusters of malignant cells and glandular pattern in dermis [H and E, ×100] and (b) dense infiltration of malignant cells [H and E, ×400] |
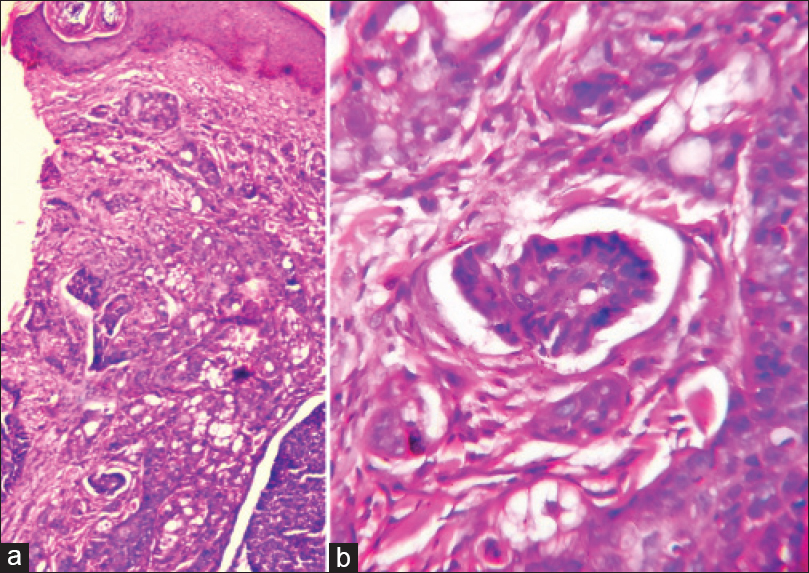 |
| Figure 3: (a) Tumor cell deposition in dermal lymphatics with mild perivascular lymphocytic infiltrate. [H and E, ×100] and (b) cluster of tumor cells within dilated lymphatic [H and E, ×400] |
Ovarian carcinoma has a rapid progression, but cutaneous involvement is quite rare at presentation and also during the course of the disease. [1] Krathen et al., in a meta-analysis of 689 patients with cutaneous metastases, showed that only 3.8% of them were of ovarian origin. [2]
Cutaneous metastases in ovarian carcinoma can be explained by: direct invasion from the underlying growth, contiguous extension of the tumor cells through lymphatics and accidental implantation of the tumor cells during surgical procedures. They can present as small nodules, erythematous lesions resembing erysipelas (also known as carcinoma erysipeloides), and cicatricial plaques. Most commonly, cutaneous involvement is limited to the abdominal skin and generally manifests as nodules near scars from previous malignancy-related surgeries. [3] Our case had two types of skin lesions: first, erythematous to dusky red papules and nodules, both at the site of surgical procedure, indicating accidental implantation of malignant cells, as well as distantly distributed over whole abdomen and breasts; second, multiple erythematous macules over the breast and upper abdomen.
Carcinoma erysipeloides, also known as inflammatory carcinoma, results from inflammation around superficial dermal lymphatics due to metastasis of malignant cells. [4] It usually manifests as erythematous patches or plaques that clinically resemble erysipelas and the resulting inflammation due to occlusion of dermal lymphatics may cause local edema, warmth, and tenderness. [5] Our patient had translucent vesicles overlying the erythematous macules at places, indicating involvement of dermal lymphatics.
It has been suggested that carcinoma erysipeloides is associated more commonly with cancers that metastasize via lymphatic spread and breast carcinoma is the most common neoplasm to incite it. [6] We were able to find only 10 previously reported cases of carcinoma erysipeloides of ovarian origin. [7],[8],[9],[10],[11] As in our patient, the most frequent histologic variant of ovarian cancer metastatic to the breast is serous adenocarcinoma. In addition, our case also had a firm nodule of 3 × 2 cm size in the right breast, which is also quite unusual with ovarian cancer, representing 6.8% of all cancers metastatic to the breast. [11]
Cutaneous metastases from ovarian or other gynecological malignancies are suggestive of advanced disease with widespread intraperitoneal involvement and invariably carry a bad prognosis. [1] Most of the time, treatments such as chemotherapy, radiotherapy or surgery are ineffective in patients with such advanced disease.
We suggest that whenever patients with ovarian carcinoma present with skin lesions resembling erysipelas or cellulitis over the abdomen, chest, or thighs, dermatologists or physicians should consider the possibility of carcinoma erysipeloides.
| 1. |
Dauplat J, Hacker NF, Nieberg RK, Berek JS, Rose TP, Sagae S. Distant metastases in epithelial ovarian carcinoma. Cancer 1987;60:1561-6.
[Google Scholar]
|
| 2. |
Krathen RA, Orengo IF, Rosen T. Cutaneous metastasis: A meta-analysis of data. South Med J 2003;96:164-7.
[Google Scholar]
|
| 3. |
Cormio G, Capotorto M, Vagno GD, Cazzolla A, Carriero C, Selvaggi L. Skin metastases in ovarian carcinoma: A report of nine cases and a review of the literature. Gynecol Oncol 2003;90:682-5.
[Google Scholar]
|
| 4. |
Lever LR, Holt PJ. Carcinoma erysipeloides. Br J Dermatol 1991;124:279-82.
[Google Scholar]
|
| 5. |
Lee B, Tannenbaum N. Inflammatory carcinoma of the breast. Surg Gynecol Obstet 1924;39:580-95.
[Google Scholar]
|
| 6. |
Cox SE, Cruz PD Jr. A spectrum of inflammatory metastasis to skin via lymphatics: Three cases of carcinoma erysipeloides. J Am Acad Dermatol 1994;30:304-7.
[Google Scholar]
|
| 7. |
Schonmann R, Altaras M, Biron T, Bernheim J, Fishman A. Inflammatory skin metastases from ovarian carcinoma-a case report and review of the literature. Gynecol Oncol 2003;90:670-2.
[Google Scholar]
|
| 8. |
Sato T, Muto I, Fushiki M, Hasegawa M, Hasegawa M, Sakai T, et al. Metastatic breast cancer from gastric and ovarian cancer, mimicking inflammatory breast cancer: Report of two cases. Breast Cancer 2008;15:315-20.
[Google Scholar]
|
| 9. |
Klein RL, Brown AR, Gomez-Castro CM, Chambers SK, Cragun JM, Grasso-Lebeau L, et al. Ovarian cancer metastatic to the breast presenting as inflammatory breast cancer: A case report and literature review. J Cancer 2010;1:27-31.
[Google Scholar]
|
| 10. |
Gingell D, Samuel A, Haynik D, McBee W, Kelley J, Zorn K, et al. Metastatic ovarian serous carcinoma presenting as inflammatory breast cancer: A case report. Int J Gynecol Pathol 2010;29:243-7.
[Google Scholar]
|
| 11. |
Puig VG, Frangos J, Hollmann TJ, Peterson SD, Matulonis U, Lipworth AD. Rash in a Patient with Ovarian Cancer: Carcinoma Erysipeloides of the Breast in a Patient with Advanced Ovarian Carcinoma. Clin Infect Dis 2012;54:575-6.
[Google Scholar]
|
Fulltext Views
4,857
PDF downloads
2,433





![[Figure - 1]](#fig_ijdvl_2015_81_4_425_158662_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2015_81_4_425_158662_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2015_81_4_425_158662_f3.jpg){kind=link}