Translate this page into:
Extramammary Paget's disease
Correspondence Address:
Manas Chatterjee
Classified Specialist (Dermatology and STD), Military Hospital, Jodhpur-342006, Rajasthan.
India
| How to cite this article: Banerjee S, Chatterjee M, Chand K. Extramammary Paget's disease. Indian J Dermatol Venereol Leprol 2005;71:417-420 |
Abstract
Two patients with extramammary Paget's disease are being reported. The first case was a 60-year-old male who presented with gradually progressive pruritic ulcerated lesion over perianal region not responding to various topical medications. Dermatological examination revealed a large erythematous sharply marginated scaly plaque in the perianal region extending into the anal canal, covered with grayish crusts and shallow erosions. Skin biopsy from the lesion was suggestive of Paget's disesase. The second patient, a 60-year-old male, with a three year long history, presented with similar lesions and findings. Skin biopsy in this case was also consistent with Paget's disease. These two cases of extramammary Paget's disease involving the perianal region are being reported because of their rarity and also to stress the fact that a high degree of suspicion is needed for the diagnosis of this uncommon disease entity. |
|
 |
|
 |
|
 |
|
Introduction
Extramammary Paget′s disease [EMPD] is defined as a marginated plaque resembling Paget′s disease [PD] clinically and histologically, but occurring in the genital region, axilla or most commonly, vulva.[1] It is a rare disease occurring more frequently in women and usually starting in the fifth decade of life or thereafter. Since Sir James Paget′s original description, extramammary Paget′s disease has been surrounded by controversy, speculation and much interest on the part of surgeons, pathologists and dermatologists.[2] The significance of this disease lies in the fact that the innocuous cutaneous lesion may be an ominous harbinger of underlying malignancy. Although the clinical and histological features of mammary Paget′s disease are well established, the source of neoplastic cells in EMPD remains controversial.
We report two cases of EMPD in the perianal region who had long-standing symptomatology.
Case History
Case 1 A 60-year-old male, an old case of cerebrovascular accident, type II diabetes mellitus and hypertension presented with a pruritic ulcerated lesion over the perianal region of two years′ duration. It initially started as a small plaque that slowly but relentlessly progressed, despite various topical medications. There was no history of bowel or bladder disturbances.
Dermatological examination revealed a 20x15 cm sharply marginated and rounded raised plaque enclosing a red erythematous scaly area in the perianal region. It was covered with greyish crusts and shallow erosions that extended into the anal canal. The surface showed pinpoint bleeding points with purulent discharge [Figure - 1]. Proctoscopy revealed that the lesion extended a few centimeters inside the anal canal. There was no regional lymphadenopathy.
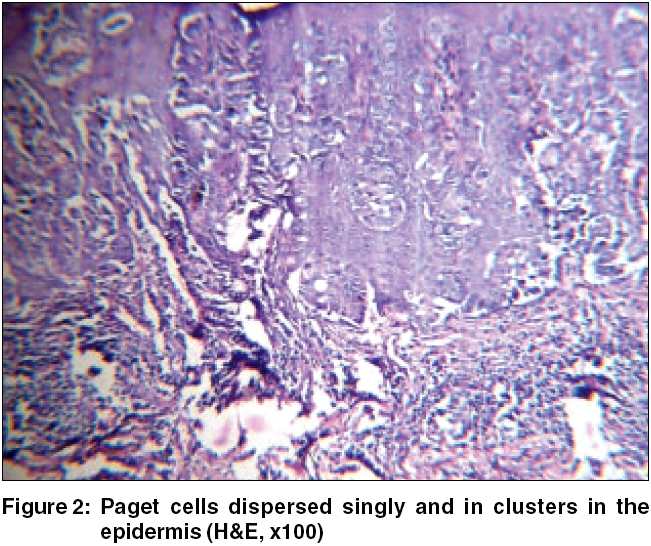
Contrast enhanced Computerized Tomography scan of the abdomen did not reveal any intra-abdominal mass or retroperitoneal lymph nodes. Skin biopsy from the lesion showed numerous Paget′s cells lying singly and in clusters in the epidermis and also infiltrating along the skin appendages [Figure - 2] [Figure - 3]. Dermis showed chronic inflammatory cells with invasion of Paget′s cells into the dermis at places. Periodic acid-Schiff (PAS) and alcian blue stains were positive.
The patient was referred to an oncosurgeon for further management and is now undergoing radiotherapy.
Case 2 A 65-year-old man presented with a pruritic ulcerated plaque over the perianal region of three years′ duration. The lesion was insidiously progressive despite all topical therapy. There was no history of alteration of bowel and bladder habits.
Dermatological examination revealed a well-defined erythematous raised plaque with well-delineated erythematous raised borders with shallow erosions and grey crusts. The lesion measured about 25x20 cm circumferentially around the perianal region and extended into the anal canal. The surface showed pinpoint bleeding with serosanguinous discharge [Figure - 4]. The findings of skin biopsy were consistent with Paget′s disease. The patient was referred to an oncosurgeon for further management and is presently undergoing radiotherapy.
Discussion
EMPD is a rare disease. It occurs more frequently in women than in men and starts usually in the fifth decade or thereafter.[1] It has a predilection for areas with a high density of apocrine glands such as the vulva, penis, scrotum, anus, perianal region and axilla.
The common presenting features include pruritus, bleeding, oozing, tenderness, painful burning sensation or hypopigmented/eczematous lesions.[3] Lesions may grossly appear flaky or white and may also resemble squamous cell carcinoma in situ, melanoma or benign dermatosis. The hallmark is relentless progression despite topical therapy and the sharp raised margin.
There are usually three patterns of EMPD: (a) an in situ epithelial form without associated carcinoma, (b) an epithelial form with associated adnexal carcinoma, and (c) associated with visceral malignancy of either genitourinary or the gastrointestinal tract.[4] EMPD cells themselves also have the potential to invade the dermis and to metastasize. The adnexal carcinomata reported include apocrine, eccrine, sebaceous gland carcinoma and carcinoma of ceruminous glands.
There is a strong association between the presenting anatomical site of EMPD and the underlying visceral carcinoma.[5] Helwig and Graham reported a frequency of visceral carcinoma associated with perianal EMPD in the range of almost 86%.[4] The frequency is much lower in vulval EMPD; this difference may be reflective of differences in the lymphatic drainage and indistinct boundaries in the perianal region. The characteristic histology of EMPD is Paget′s cells, which consist of distinct intraepithelial mucus-secreting neoplastic proliferative cells with abundant pale staining cytoplasm and large atypical nuclei. Sialomucin, a nonsulfated acid mucopolysaccharide, is found in the cytoplasm of Paget′s cells. It usually stains with colloidal iron, alcian blue, mucicarmine E and PAS stains. It is resistant to diastase and bovine testicular hyaluronidase. Immunohistochemical staining includes carcinoembryonic antigen for Paget′s disease.[5]
The histogenesis and pathogenesis of EMPD are controversial. The current theories of origin of Paget′s cells are: (a) an adenocarcinoma originating multifocally in pluripotent epidermal cells, (b) an underlying adenocarcinoma of the apocrine, eccrine and sweat glands, or (c) the multicentric effect of a carcinogenic stimulus in the epidermis.[4] Paget cells in mammary and extramammary Paget′s disease seem to have different origins, i.e. those of mammary Paget′s disease ascend to the epidermis from lactiferous ducts, whereas those of extramammary Paget′s disease originate in the epidermis itself.[6]
The differential diagnosis in the anogenital area includes neurodermatitis, psoriasis, seborrheic dermatitis, lichen simplex, lichen planus, mycosis fungoides, Bowen′s disease and periorificial tuberculosis.[4] Histopathologically, the differential diagnosis includes pagetoid Bowen′s disease and pagetoid malignant melanoma in situ.[7]
The treatment of choice for EMPD is surgical excision, although other modes of therapy, including radiation, dissection, curettage, topical 5-FU, and cryosurgery have been employed. Despite varied modalities of therapy, local recurrence is a significant problem, to the extent of 33%. Multifocal involvement and difficulty in clinical delineation of cutaneous margins are major factors in relapse and chronicity of the disease.[8] According to some authors, non-surgical modalities should be considered in place of surgery as the primary treatment for non-invasive perianal Paget′s disease, with radical surgery being reserved for failures or invasive disease.[9]
The prognosis depends on whether the disease extends beyond the epidermis and the adnexal epithelium. If it is associated with subjacent adnexal carcinoma or regional visceral carcinoma, the prognosis is poor, with Helwig and Graham reporting a death rate of 83% in one series.[4]
To conclude, the key to diagnosis of EMPD is a high degree of suspicion. Any eczematous or thickened area where apocrine glands are normally encountered and which does not resolve with appropriate therapy should arouse the suspicion of Paget′s disease.
| 1. |
MacKie RM. Epidermal skin tumours. In: Champion RH, Burton JL, Burns DA Breathnach SM, editors. Rook/ Wilkinson/ Ebling Textbook of dermatology. 6th ed. Oxford: Blackwell Science; 1998. p. 1678-9.
[Google Scholar]
|
| 2. |
Jabbar AS. Perianal extramammary Paget's disease. Eur J Surg Oncol 2000;26:612-4.
[Google Scholar]
|
| 3. |
Balducci L, Crawford ED, Smith GF, Lambuth B, McGehee R, Hardy C. Extramammary Paget's disease: An annotated review. Cancer Invest 1988;6:293-303.
[Google Scholar]
|
| 4. |
Helwig EB, Graham GH. Anogenital (extramammary) Paget's disease. A clinicopathologic study. Cancer 1963;16:387-403.
[Google Scholar]
|
| 5. |
Chanda JJ. Extramammary Paget's disease: Prognosis and relationship to internal malignancy. J Am Acad Dermatol 1985;13:1009-14.
[Google Scholar]
|
| 6. |
Sitakalin C, Ackerman AB. Mammary and extramammary Paget's disease. Am J Dermatopathol 1985;7:335-40.
[Google Scholar]
|
| 7. |
Kirkham N. Tumours and cysts of the epidermis. In: Elder D, Elenitsas R, Jaworksy C, Johnson B Jr, editors. Lever's Histopathology of the skin. 8th ed. Philadelphia: Lippincott-Raven; 1997. p. 736-8.
[Google Scholar]
|
| 8. |
Burrows NP, Jones DH, Hudson PM, Pye RJ. Treatment of extramammary Paget's disease by radiotherapy. Br J Dermatol 1995;132:970-2.
[Google Scholar]
|
| 9. |
Tulchinsky H, Zmora O, Brazowski E, Goldman G, Rabau M. Extramammary Paget's disease of the perianal region. Colorectal Dis 2004;6:206-9.
[Google Scholar]
|
Fulltext Views
5,627
PDF downloads
3,820





![[Figure - 1]](#fig_ijdvl_2005_71_6_417_18948_1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2005_71_6_417_18948_2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2005_71_6_417_18948_3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2005_71_6_417_18948_4.jpg){kind=link}