Translate this page into:
Facial cellulitis and Ludwig's angina associated with calcium hydroxylapatite injection in an immunocompetent patient
2 Department of Dermatology and Allergy, Technische Universität München, Munich, Germany
3 Department of Radiology, Kaohsiung Veterans General Hospital, Taiwan
Correspondence Address:
Kai-Che Wei
Department of Dermatology, Kaohsiung Veterans General Hospital, No. 386, Dazhong First Road, Zo-Ying Dist., Kaohsiung, 813
Taiwan
| How to cite this article: Jang CS, Chen WC, Fu JH, Wu CS, Wei KC. Facial cellulitis and Ludwig's angina associated with calcium hydroxylapatite injection in an immunocompetent patient. Indian J Dermatol Venereol Leprol 2016;82:112 |
Sir,
A 30-year-old female presented to us with swelling, local rise of temperature and tenderness on her right lower cheek two weeks following a local injection of calcium hydroxylapatite filler for facial lifting. A gradual downward and lateral extension of the erythema and swelling was observed in the following week which involved the submental and submandibular regions and the upper neck [Figure - 1]a and [Figure - 1]b. This occurred despite administering oral antibiotics including cefadroxil, amoxicillin and rifampicin. A CT scan revealed a soft tissue swelling in the right cheek, masticator space, buccal space, bilateral submandibular and submental regions [Figure - 1]c and [Figure - 1]d. Dental examination showed no evidence of odontogenic infection. A clinical diagnosis of deep neck space infection was made. The patient was started on intravenous ampicillin/sulbactam (3 g every 6th hourly) for 12 days, following which the swelling and tenderness gradually subsided. A follow up CT scan after two months revealed complete resolution of the soft tissue inflammation. No recurrence was noted one year after completion of therapy.
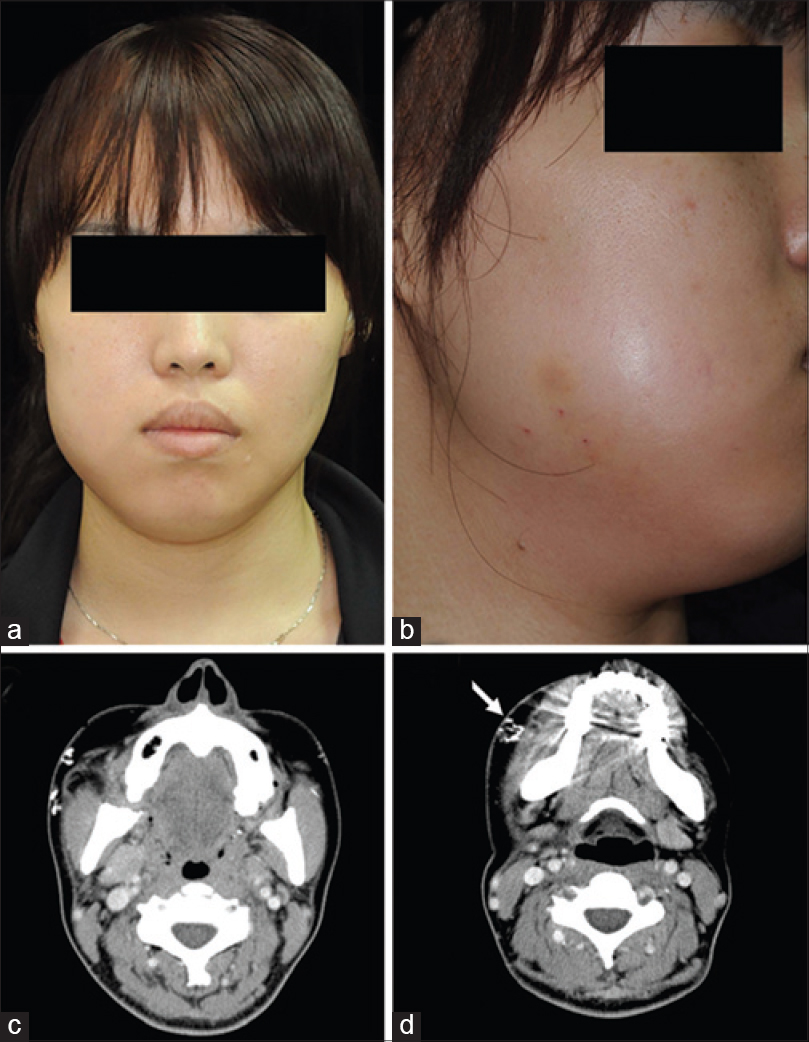 |
| Figure 1: (a and b) Swelling over the right cheek, submental and submandibular regions and upper neck 2 weeks following the filler injection. (c and d) CT scan image showing soft tissue swelling in the right masticator space, buccal space and submandibular regions. Multiple hyper-dense globules and clumps in the skin over the bilateral mid-face region, consistent with calcium hydroxylapatite deposition (white arrow) |
The incidence of complications associated with calcium hydroxylapatite fillers is low. The most common complications are pain, erythema, bruising and nodules. Infection is uncommon, and we were unable to find any previous reports of deep neck space infection.[1],[2] The most devastating complication is descending necrotizing fasciitis, which requires early diagnosis and aggressive treatment. Odontogenic infections are the most common cause of deep neck space infection.[3],[4] Skin infections seldom cause deep neck space infection, and it has been reported to occur in 7 of 80 patients in one study,[3] and 1 of 185 patients in another.[4] Deep neck space infection associated with filler injection is considered to be extremely rare. We were able to find only one previous report of deep facial abscess following dermal filler injection in the English literature.[5] Fever, swelling, local rise of temperature and tenderness are the typical presentations of deep neck space infections, as seen in our patient. Satisfactory response to intravenous antibiotics confirms the diagnosis. Although surgical drainage is the mainstay of therapy, conservative medical management does not increase mortality or length of hospitalization in uncomplicated cases.[6]
CT scan imaging is a useful tool to differentiate deep neck space infections from non-infected facial swellings. Three dimensionally reconstructed CT scan images can further reveal the severity and extent of involvement, which is critical for treatment selection. The CT scan report in our case indicated the location and distribution of the filler as well. Calcium hydroxylapatite has radiographic features similar to the bone mineral matrix, with attenuation values typically in the range of 280–700 HU (Hounsfield units).[7] In two dimensional axial CT scans, it can be observed as hyper-dense clumps within soft tissue, with a density similar to that of compact bone [Figure - 2]a. A three dimensional image reconstructed from the original CT data can reveal the location and techniques adopted during the calcium hydroxylapatite filler injection. In our case, linear streaks over the bilateral infraorbital areas (tear trough) and several lumps over the bilateral zygomatic areas and cheeks were identified in the reconstructed CT image [Figure - 2]b,[Figure - 2]c,[Figure - 2]d. It indicated that the patient had received calcium hydroxylapatite injections for peri-orbital augmentation, facial lifting and jaw line contouring. The cross-linked network shape of the filler implied that fanning and cross hatching injection techniques had been used over both cheeks.
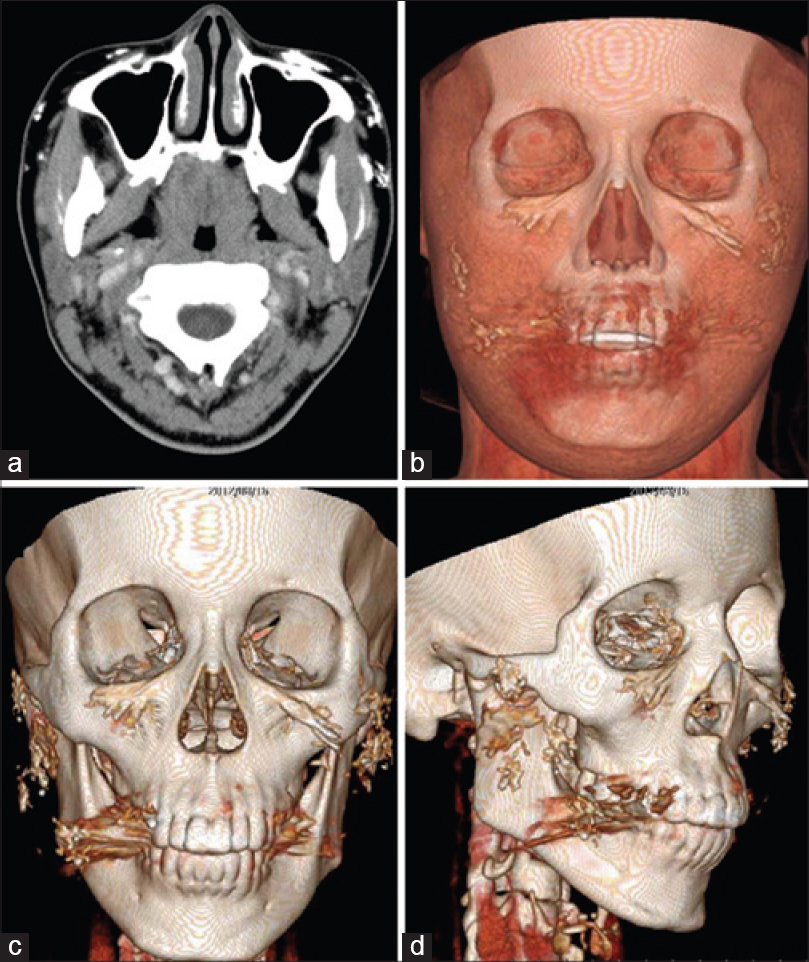 |
| Figure 2: (a) Calcium hydroxylapatite can be identified in the original two dimensional axial CT scan(white arrow). (b and c) Three dimensionally reconstructed image shows linear streaks over the bilateral infraorbital areas indicating the usage of threading technique. (c and d) The cross linked network shape of the filler over the zygomatic areas and cheek indicates the usage of the fanning or cross-hatching techniques for facial lifting |
Three dimensional CT reconstruction is a useful tool for the early diagnosis of such infections, and it can also be used to reveal the filler injection sites and techniques.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
| 1. |
Daines SM, Williams EF. Complications associated with injectable soft-tissue fillers: A 5-year retrospective review. JAMA Facial Plast Surg 2013;15:226-31.
[Google Scholar]
|
| 2. |
Pavicic T. Calcium hydroxylapatite filler: An overview of safety and tolerability. J Drugs Dermatol 2013;12:996-1002.
[Google Scholar]
|
| 3. |
Suehara AB, Goncalves AJ, Alcadipani FA, Kavabata NK, Menezes MB. Deep neck infection: Analysis of 80 cases. Braz J Otorhinolaryngol 2008;74:253-9.
[Google Scholar]
|
| 4. |
Huang TT, Liu TC, Chen PR, Tseng FY, Yeh TH, Chen YS. Deep neck infection: Analysis of 185 cases. Head Neck 2004;26:854-60.
[Google Scholar]
|
| 5. |
Rousso JJ, Pitman MJ. Enterococcus faecalis complicating dermal filler injection: A case of virulent facial abscesses. Dermatol Surg 2010;36:1638-41.
[Google Scholar]
|
| 6. |
Plaza-Mayor G, Martinez-San Millan J, Martinez-Vidal A. Is conservative treatment of deep neck space infections appropriate? Head Neck 2001;23:126-33.
[Google Scholar]
|
| 7. |
Ginat DT, Schatz CJ. Imaging features of midface injectable fillers and associated complications. AJNR Am J Neuroradiol 2013;34:1488-95.
[Google Scholar]
|
Fulltext Views
4,586
PDF downloads
2,685





![[Figure - 1]](#fig_ijdvl_2016_82_1_112_162322_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2016_82_1_112_162322_f2.jpg){kind=link}