Translate this page into:
Follicular psoriasis - dermoscopic features at a glance
2 Department of Pathology, JIPMER, Puducherry, India
Correspondence Address:
Rashmi Kumari
Department of Dermatology, Venereology and Leprology, JIPMER, Puducherry - 605 006
India
| How to cite this article: Behera B, Gochhait D, Remya R, Resmi M R, Kumari R, Thappa DM. Follicular psoriasis - dermoscopic features at a glance. Indian J Dermatol Venereol Leprol 2017;83:702-704 |
Sir,
A 34-year-old-female presented with multiple asymptomatic-to-mildly itchy skin-colored-to-reddish elevated lesions involving both her lower limbs for last 2 months. There was no history suggestive of upper respiratory, gastrointestinal or urinary tract infection. She denied any history of prior drug intake, scalp scaling, joint pain or swelling, or palmo-plantar thickening. Cutaneous examination revealed multiple discrete, erythematous follicular scaly papules over her both thighs and lower legs [Figure - 1]. Mucosa, nails, scalp, palms, and soles were spared. All systemic examinations were within normal limits. Follicular psoriasis, malassezia folliculitis, and follicular lichen planus were considered as the differentials. Dermoscopic examination under nonpolarized contact dermoscopy (Heine Delta20® Dermatoscope, 10× magnification) revealed a white-brown background/homogenous area, normal looking terminal hair at the centre, perifollicular scaling, multiple red dots/dotted vessels, red globules, twisted red loops, and glomerular vessels/bushy capillaries [Figure - 2]. Histopathological examination of a papule revealed a dilated follicular opening, parakeratotic follicular plugging, follicular hyperkeratosis, perifollicular confluent parakeratosis, hypogranulosis, Munro-micro abscess, suprapapillary thinning, upper dermal dilated and tortuous blood vessels, and mild perivascular lympho-histiocytic and neutrophilic infiltration [Figure - 3]. Based on these findings, a diagnosis of follicular psoriasis was made and the patient was advised treatment with a topical application of a combination of calcipotriol (0.005% w/w) and clobetasol (0.05% w/w) ointment.
 |
| Figure 1: Multiple, discrete, erythematous scaly papules over the left lower leg |
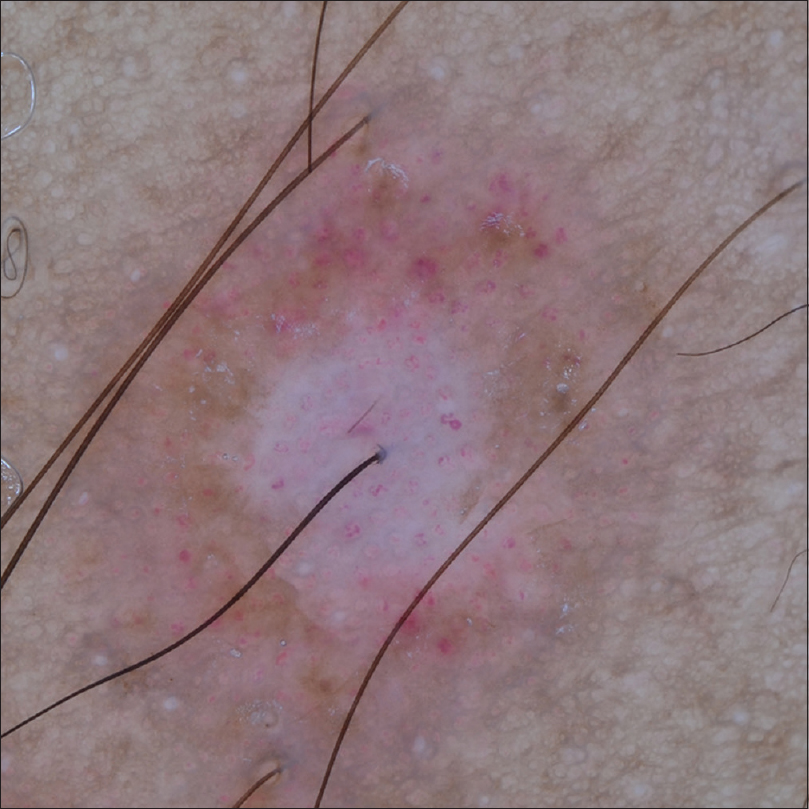 |
| Figure 2: Nonpolarized contact dermoscopy showing perifollicular white homogenous area, central normal looking terminal hair, perifollicular scaling, multiple red dots/dotted vessels, red globules, twisted red loops, and glomerular vessels/bushy capillaries |
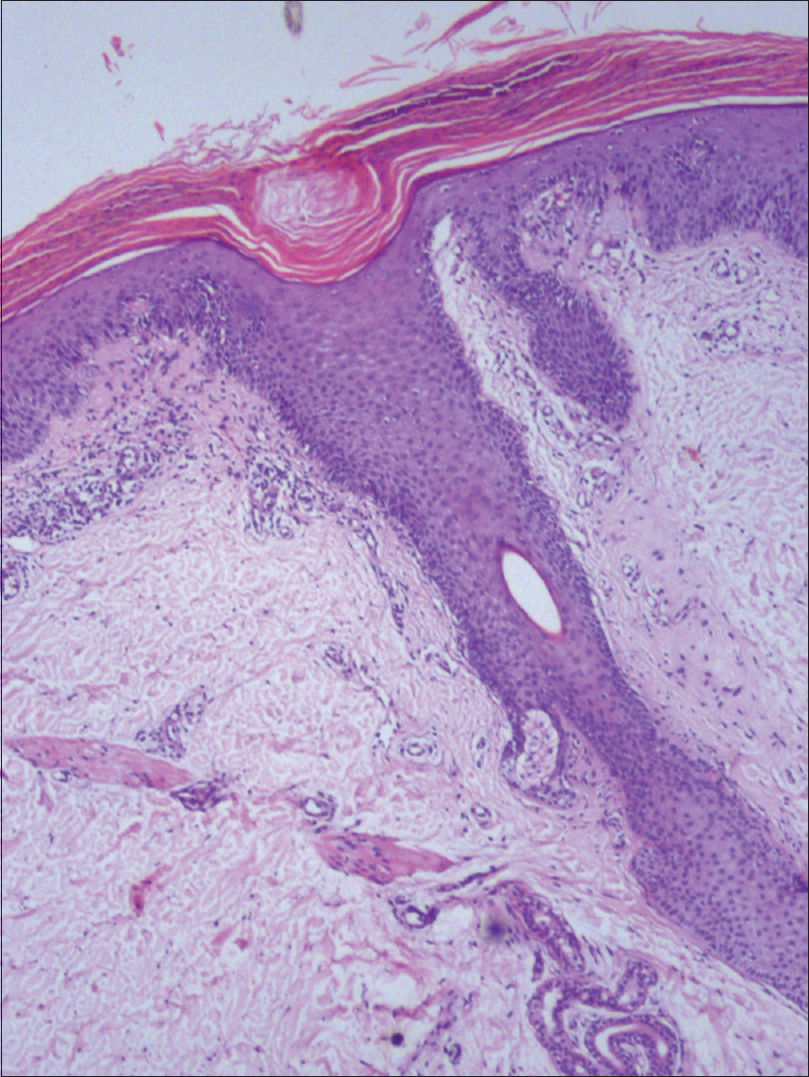 |
| Figure 3: Histopathology showing features of follicular psoriasis. (H and E, ×100) |
Follicular psoriasis is an under-recognized entity that affects adults more commonly than children without any sexual predilection. Amongst the two clinical subtypes, the adult form commonly affects females and presents as multiple, discrete, follicle-based, hyperkeratotic papules predominantly over the thigh, as in our case. The second type commonly affects children and present as asymmetric, grouped, follicular, keratotic papules predominantly affecting the trunk, axilla, and extensor aspect of limbs.[1]
The role of dermoscopy as a diagnostic tool is gaining importance with time as more diseases are being reported where dermoscopy can play a role not only in their diagnosis but also in monitoring their course. To the best of our knowledge dermoscopic features of follicular psoriasis have not yet been reported in the literature. The various dermoscopic features described for plaque psoriasis are white scale, symmetrically and regularly distributed dotted vessels on a light or dull red background, red globular rings, twisted loops, and glomerular or bushy vessels.[2] The present case shows all these dermoscopic features thus suggesting similar dermoscopic findings for different morphological variants of psoriasis. The dermoscopic features described for scalp seborrheic dermatitis are fine yellowish scale, patchy dotted vessels/red dots, red globules, arborizing vessels, and atypical vessels.[2] The dermoscopic features described for other inflammatory conditions mimicking follicular psoriasis are; atopic dermatitis [yellowish scales (with or without white scales) and patchy dotted vessels], pityriasis lichenoides chronica [nondotted vessels (i.e. milky red areas/globules, linear irregular and branching vessels), focally distributed dotted vessels and orange-yellowish structureless areas] and papular pityriasis rosea (patchy dotted vessel, peripheral white scale).[2],[3]
The dermoscopic features described for various follicular dermatoses that may mimic follicular psoriasis (especially the second type) are keratosis pilaris (irregular twisted or coiled vellus hair embedded in the horny layer, perifollicular erythema, scaling, and pigmentation), follicular lichen planus (follicular plug without broken or twisted hairs), pityriasis rubra pilaris (white keratotic plug, yellow peripheral keratotic ring, perifollicular erythema, and linear vessels), scurvy (whitish hair follicles with “corkscrew” hair surrounded by a hemorrhagic violaceous halo), and perforating folliculitis (central white clod surrounded by structureless gray area and brown reticular lines under polarized dermoscopy).[4],[5],[6],[7] The presence of central keratotic plug along with altered hair morphology (twisted or coiled or broken hair) has been described for disorders of abnormal keratinization such as pityriasis rubra pilaris, keratosis pilaris, and scurvy. The presence of vascular pattern, such as diffuse dotted and glomerular vessels, may help in differentiating follicular psoriasis from these disorders. The perifollicular white homogenous area [asterix, [Figure - 2] histologically corresponds to the follicular and perifollicular hyperkeratosis and acanthosis [Figure - 3], perifollicular white scale to the perifollicular parakeratosis [Figure - 3] and the dotted and nondotted vessels to the dilated and tortuous dermal blood vessels oriented at different angles to the surface of the skin.
To conclude, the presence of central normal looking terminal hair, perifollicular white scale and homogenous area, and vascular structures such as diffuse dotted, twisted or glomerular vessels may help in differentiating follicular psoriasis from its clinical mimics.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Babino G, Moscarella E, Longo C, Lallas A, Ferrara G, Cusano F, et al. Follicular psoriasis: An under-recognized condition. J Eur Acad Dermatol Venereol 2016;30:1397-9.
[Google Scholar]
|
| 2. |
Errichetti E, Stinco G. Dermoscopy in general dermatology: A practical overview. Dermatol Ther (Heidelb) 2016;6:471-507.
[Google Scholar]
|
| 3. |
Errichetti E, Lacarrubba F, Micali G, Piccirillo A, Stinco G. Differentiation of pityriasis lichenoides chronica from guttate psoriasis by dermoscopy. Clin Exp Dermatol 2015;40:804-6.
[Google Scholar]
|
| 4. |
Panchaprateep R, Tanus A, Tosti A. Clinical, dermoscopic, and histopathologic features of body hair disorders. J Am Acad Dermatol 2015;72:890-900.
[Google Scholar]
|
| 5. |
López-Gómez A, Vera-Casaño Á Gómez-Moyano E, Salas-García T, Dorado-Fernández M, Hernández-Gil-Sánchez J, et al. Dermoscopy of circumscribed juvenile pityriasis rubra pilaris. J Am Acad Dermatol 2015;72 1 Suppl:S58-9.
[Google Scholar]
|
| 6. |
Cinotti E, Perrot JL, Labeille B, Cambazard F. A dermoscopic clue for scurvy. J Am Acad Dermatol 2015;72 1 Suppl: S37-8.
[Google Scholar]
|
| 7. |
Ramirez-Fort MK, Khan F, Rosendahl CO, Mercer SE, Shim-Chang H, Levitt JO. Acquired perforating dermatosis: A clinical and dermatoscopic correlation. Dermatol Online J 2013;19:18958.
[Google Scholar]
|
Fulltext Views
10,852
PDF downloads
1,818





![[Figure - 1]](#fig_ijdvl_2017_83_6_702_216139_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2017_83_6_702_216139_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2017_83_6_702_216139_f3.jpg){kind=link}