Translate this page into:
Giant cell arteritis with extensive scalp necrosis: A diagnostic and therapeutic challenge
Correspondence Address:
Diana Crisan
Department of Dermatology and Allergic Diseases, University of Ulm, Albert-Einstein-Allee 23, Ulm 89081
Germany
| How to cite this article: Crisan D, Schneider LA, Kastler S, Psotta-Schachtner C, Geth�ffer K, Sindrilaru A, Scharffetter-Kochanek K. Giant cell arteritis with extensive scalp necrosis: A diagnostic and therapeutic challenge. Indian J Dermatol Venereol Leprol 2016;82:539-542 |
Sir,
Giant cell arteritis, a rare systemic inflammatory vasculitis that affects the elderly, is characterized by a panarteritis of medium and large arteries especially the extracranial branches of the carotid artery. It often presents with a polymorphic, even non-specific symptomatology that leads to delayed diagnosis and treatment resulting in poor outcomes for patients.
A 78-year-old woman, who had suffered from severe temporo-parietal headaches and malaise for about a month, suddenly presented with acute loss of vision in her right eye as well as extensive painful necrotic plaques on her scalp. For her symptoms, initially, a stroke had been ruled out in the neurology department; subsequently she was started on acyclovir 7.5 mg/kg intravenously based on the clinical suspicion of herpes zoster but her condition continued to deteriorate. At this point, she was referred to our department of dermatology at the University of Ulm, Germany. We observed that she had sharply defined painful necrotic ulcers on her temporoparietal scalp; lesions were distributed bilaterally and did not follow any dermatomal pattern [Figure - 1]. The right temporal artery was visibly enlarged, indurated and extremely tender. Laboratory investigations showed an increased erythrocyte sedimentation rate of 60 mm/1 h and a slightly increased C-reactive protein of 6.6 mg/dl (normal, <5 mg/dl). Blood counts were normal except for mild normochromic anemia with 12.2 g/dl hemoglobin, (14.0–17.4 g/dl). Rheumatoid factor, perinuclear antineutrophil cytoplasmic antibody (p-ANCA), cytoplasmic antineutrophil cytoplasmic antibody (c-ANCA) and antinuclear antibody (ANA) were negative. Microbiological samples from the scalp showed physiological skin flora and no varicella-zoster virus DNA was detected. A right temporal artery biopsy showed a lympho-histiocytic infiltrate of the arterial wall as well as an obliterated lumen [Figure - 2]. Magnetic resonance imaging of the head revealed occlusion of the central retinal artery.
 |
| Figure 1: Extensive temporoparietal scalp necrosis: (a) Left parietal area; (b) view from above |
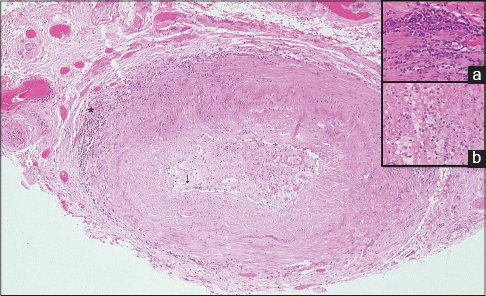 |
| Figure 2: Infiltration of the media and adventitia of the right temporal artery with inflammatory mononuclear cells. A significant intimal thickening with occlusion of the arterial lumen was observed. H and E, (×10); (a) inset from the indicated area (*), magnification (×400), (b) inset from the indicated ar(↓), magnification (×40) |
Based on the symptoms including necrotic ulcers of the scalp, loss of vision in the right eye, elevated inflammatory parameters (erythrocyte sedimentation rate, C-reactive protein) and the histopathology, the patient was diagnosed with giant cell arteritis. She was immediately treated with high-dose systemic oral corticosteroids (prednisolone 1 mg/kg) for 3 weeks followed by gradual tapering over 1 year to a maintenance dose of 5 mg/day. After 3 months of steroid therapy, methotrexate, 15 mg subcutaneously weekly was added as a steroid-sparing drug.
With treatment, the patient's clinical condition improved (no extension of scalp necrosis, disappearance of headaches and subjective clinical improvement) and the inflammatory markers also normalized within 3 weeks of therapy. We were able to surgically debride the necrotic scalp and cover the remaining defect with a mesh graft, 3 months after initiation of treatment [Figure - 3]. Unfortunately, the loss of vision in the right eye was irreversible. One year later, despite adequate prophylaxis for osteoporosis, the patient developed several vertebral fractures that required surgical treatment.
 |
| Figure 3: Mesh-grafting of the defect following scalp necrosis debridement: (a) Mesh-graft from upper thigh covering the defect; (b and c) appearance 1 year after surgery |
Giant cell arteritis is a systemic immune-mediated vasculitis affecting persons over 50 years of age, most commonly involving the branches of the external carotid artery. The etiology is controversial. The association with the HLA-DR4 haplotype indicates a genetic predisposition. Other studies suggest a possible association with chlamydia pneumonia, parvovirus B19 or herpes zoster infection.[1]
The pathogenesis involves recruitment of antigen-triggered T-cells and macrophage activation in the vessel wall leading to diffuse inflammation driven by pro-inflammatory cytokines with consequent intimal thickening, arterial stenosis and severe ischemic complications.[2]
The diagnosis is often difficult as most systemic manifestations are non-specific and scalp necrosis as seen in our patient is a rarely encountered and late event, when visual loss or other complications have already occurred.
Systemic steroid treatment with adequate side effect prophylaxis should be immediately initiated upon the suspicion of giant cell arteritis as it stops disease progression and prevents the development of potentially severe complications.[3]
We were able to find about 100 case reports of giant cell arteritis manifesting with severe scalp necrosis in the literature; our case highlights this seldom seen but very severe presentation, where prompt recognition and therapy are crucial to prevent the patient from developing a permanent visual loss or further complications. Many cases of giant cell arteritis are misdiagnosed as herpes zoster and inappropriate treatment leads to disease progression and the development of severe irreversible complications. According to previous reports, the presence of scalp necrosis in temporal arteritis represents a poor prognostic factor being associated with greater mortality and an increased incidence of visual loss.[4]
Our case also illustrates certain important issues in the management of such patients since steroid therapy, although still the first-line therapy for this disease, may cause severe and long-lasting side effects. Recently published case reports describe good responses to treatment with a humanized monoclonal anti-interleukin-6-receptor antibody, tocilizumab.[5] This may be a future alternative to glucocorticoid therapy in giant cell arteritis helping to avoid significant side effects such as severe osteoporosis with pathologic vertebral fractures, as seen in our patient.
Patients with giant cell arteritis require long-term, even life-long immunosuppressive therapy with an interdisciplinary approach depending on the affected arterial branches, disease severity and overall health. Early suspicion and treatment of this condition are crucial as late diagnosis results in severe complications and high morbidity.
Acknowledgment
We are indebted to PD Dr. Med. Frank Leithäuser, Institute of Pathology, University Clinic Ulm, for preparing the histologic sections that we submitted.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Wagner AD, Gérard HC, Fresemann T, Schmidt WA, Gromnica-Ihle E, Hudson AP, et al. Detection of Chlamydia pneumoniae in giant cell vasculitis and correlation with the topographic arrangement of tissue-infiltrating dendritic cells. Arthritis Rheum 2000;43:1543-51.
[Google Scholar]
|
| 2. |
Samson M, Audia S, Martin L, Janikashvili N, Bonnotte B. Pathogenesis of giant cell arteritis: New insight into the implication of CD161+T cells. Clin Exp Rheumatol 2013;31 1 Suppl 75:S65-73.
[Google Scholar]
|
| 3. |
Suárez Cuervo C, Colunga Argüelles D, Mendoza Pacas GE, Díaz López B. Bilateral scalp necrosis in a patient with giant-cell arteritis. Med Clin (Barc) 2014;142:46.
[Google Scholar]
|
| 4. |
Tsianakas A, Ehrchen JM, Presser D, Fischer T, Kruse-Loesler B, Luger TA, et al. Scalp necrosis in giant cell arteritis: Case report and review of the relevance of this cutaneous sign of large-vessel vasculitis. J Am Acad Dermatol 2009;61:701-6.
[Google Scholar]
|
| 5. |
Oliveira F, Butendieck RR, Ginsburg WW, Parikh K, Abril A. Tocilizumab, an effective treatment for relapsing giant cell arteritis. Clin Exp Rheumatol 2014;32 3 Suppl 82:S76-8.
[Google Scholar]
|
Fulltext Views
3,530
PDF downloads
1,409





![[Figure - 1]](#fig_ijdvl_2016_82_5_539_182976_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2016_82_5_539_182976_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2016_82_5_539_182976_f3.jpg){kind=link}