
Translate this page into:
Half and half nails associated with erythema multiforme
Corresponding author: Dr. Lina Bessaad, Department of Dermatology, The Military Hospital of Tunis, Tunis, Tunisia. bessaadlina7@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Bessaad L, Rabhi F, Jaber K, Dhaoui R. Half and half nails associated with erythema multiforme. Indian J Dermatol Venereol Leprol. doi: 10.25259/IJDVL_1570_2024
Dear Editor,
Half-and-half nails were described for the first time in 1963 by Dr. Bean.1 In 1967, Dr. Philip G. Lindsay coined the term “half-and-half nails” to describe the changes in nail colour found in some patients with azotemia.1 It is a nail modification characterised by the presence of two clearly delimited bands with different colours.2 This sign is observed mainly in chronic diseases. Other causes, such as viral pathology and medication have also been associated. Half-and-half nails have not been reported in patients with erythema multiforme.
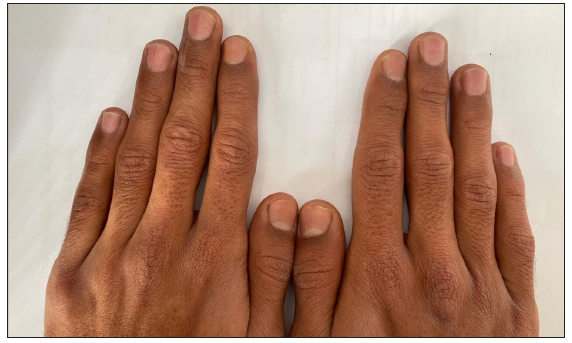
A 26‐year‐old man presented with a one-week history of asymptomatic skin eruptions of distal extremities with changes in the nails. He had no significant family history and denied consumption of drugs, tobacco or alcohol for a long period. There was a history of labial herpes four days before. Clinical examination revealed symmetrically distributed, distinct targetoid lesions on the hands and feet [Figure 1a]. The examination of the mucous membranes showed no abnormalities. All the nails were affected; each with two parts: a proximal white and a distal red, occupying approximately 40% of the nail bed with a clear line of demarcation between them [Figures 1b and 1c]. These lesions did not disappear under pressure. There were no renal or hepatic abnormalities. The COVID-19 polymerase chain reaction (PCR), and mycoplasma and HIV serologies were negative. A skin biopsy showed keratinocyte necrosis, mild superficial dermal edema, and a lymphocytic infiltrate with exocytosis in the epidermis [Figure 2]. He was diagnosed as having half-and-half nails associated with erythema multiforme and treated with systemic corticosteroids at a dose of 0.5 mg/kg/day for 7 days, with a rapidly tapering regimen. His nails improved spontaneously after two months of follow-up and without recurrence after one year [Figure 3].

- Targetoid lesions on the palm.

- Half-and-Half nails. The distal red part of the fingernails.

- Half and Half nails. Distal red part of the toenails.
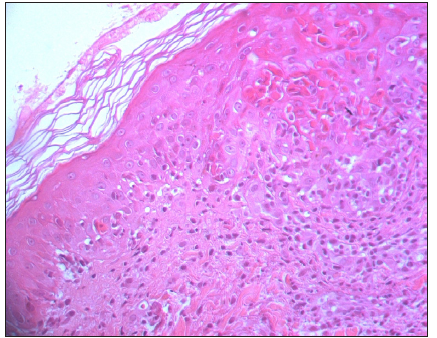
- Keratinocyte necrosis, mild superficial dermal edema, and a lymphocytic infiltrate with exocytosis in the epidermis. (Haematoxylin and eosin, 40x).
- Resolution of nail changes observed during follow-up
Erythema multiforme is an immune-mediated mucocutaneous disorder characterised by symmetrically distributed targetoid lesions which may be accompanied by mucosal erosions. It is considered a hypersensitivity reaction triggered by infections or the use of certain medications. Nail changes are uncommon. Oedema of the nail folds, onycholysis, and subsequent onychodystrophy has been described. A case of erythronychia has also been reported in a 26-year-old patient with acral erythema multiforme and erythematous areas in the nail bed adjacent to skin lesions on the back of the hands.3 Half-and-half nails is characterised by a white proximal portion and a pink, red, or brown distal portion occupying more than 20% of the nail.4 The line of demarcation between the two halves is sharp, and the colouration does not fade with pressure or change with nail growth. Half-and-half nails are seen mainly in patients with chronic kidney disease, especially with those undergoing haemodialysis, Behçet disease, Crohn disease, pellagra, Kawasaki disease, cirrhosis, and hepatocellular carcinoma, after chemotherapy and after anti-tuberculosis treatment. Viral causes, like cases of association with HIV or COVID-19 infection, have been reported, and these nail changes were considered by some authors to indicate the severity of the infection.5 In the literature, half-and-half nails have not been associated with hand, foot, and mouth disease in adults. However, they can even be seen in healthy people.6 To the best of our knowledge, no case of association of erythema multiforme and half-and-half nails have been reported. In our case, the erythema multiforme was considered an aetiology of half-and-half nails. In fact, the appearance of the nail changes concomitantly with cutaneous signs and their resolution after the healing of erythema multiforme lesions confirm the hypothesis of an association between the two entities. The role of herpes infection was not considered because of the absence of half-and-half nails with previous herpes infections. The proposed aetiology of half-and-half nails in chronic renal failure is an increase in the stimulation of melanocytes by uremic substances, which promotes the production of melanin in the distal half of the nail.2 In our case, the acute appearance of this sign in a healthy patient can be explained by the acral inflammatory process that causes vessel dilatation, which may induce a transient matrix injury; an increase in capillary density, and thickening of the capillary wall.5
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
References
- Longitudinal half-and-half nails: Case report and review. Skin Appendage Disord. 2018;4:331-4.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Under-reported finding in acral erythema multiforme. Indian J Dermatol. 2015;60:636.
- [Google Scholar]
- Half-and-half nails in a patient with graves disease. Am J Med. 2021;134:e209-10.
- [CrossRef] [PubMed] [Google Scholar]
- Half and half nail, is it a marker of severe COVID-19 infection? Ann Med Surg (Lond). 2021;71:102963.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Half and half nails in a healthy person. Acta Dermatovenerol Croat. 2017;25:303-4.
- [PubMed] [Google Scholar]




