Translate this page into:
"Human immunodeficiency virus serostatus disclosure-Rate, reactions, and discrimination": A cross-sectional study at a rural tertiary care hospital
2 Department of Preventive and Social Medicine, S. R. T. Rural Medical College & Hospital, Ambajogai (Dist-Beed), India
3 Department of Community Medicine, Jawaharlal Nehru Medical College & A. V. B. Rural Hospital, Sawangi (Meghe), Wardha, Maharashtra, India
Correspondence Address:
Umesh S Joge
Department of Preventive and Social Medicine, Government Medical College & Hospital, Akola, Maharashtra (MH)
India
| How to cite this article: Joge US, Deo DS, Choudhari SG, Malkar VR, Ughade HM. "Human immunodeficiency virus serostatus disclosure-Rate, reactions, and discrimination": A cross-sectional study at a rural tertiary care hospital. Indian J Dermatol Venereol Leprol 2013;79:135 |
Abstract
Background: From the moment scientists identified Human Immunodeficiency Virus/Acquired Immunodeficiency Syndrome (HIV/AIDS), social responses of fear, denial, stigma, and discrimination have accompanied the epidemic. Aims: To assess the rate of disclosure of HIV serostatus, reactions by the HIV/AIDS patients and their spouse, and discrimination faced by the patients. Methods: The present cross-sectional study was conducted at Antiretroviral Therapy (ART) center of a rural tertiary care hospital, situated in Marathawada region of Maharashtra state from November 2008 to October 2010. Totally, 801 HIV-positive patients coming to ART center for treatment were included after ensuring confidentiality and taking informed consent. A preformed questionnaire was used to enquire about reaction after diagnosis, disclosure, and discrimination faced by the patients. The data analyzed using descriptive statistics and Chi-square test. Results: The most common immediate reaction by the HIV patients after getting diagnosed as seropositive was fear (593, 74.03%) followed by depression (385, 48.06%) and suicidal thoughts (98, 12.25%). Out of 801 patients, 769 (96%) had spouse and of these maximum number of patients (653, 84.92%) had disclosed HIV status to their spouses. Most common immediate reaction by spouse after disclosure was crime (324, 42.13%) followed by horror (294, 38.23%) and anger (237, 36.29%). Maximum number of patients were discriminated by friends (120, 71.01%) followed by discrimination at workplace (49, 67.12%), by neighbors (32, 56.14%), and by relatives (53, 43.80%). Conclusion: Male positives were granted greater acceptance, care, and support by their spouses. More percentage of females discriminated by neighbors, relatives, and friends and at workplace which might be due to factors like customs, morals, and taboos.Introduction
Acquired immunodeficiency syndrome (AIDS) is an unprecedented public health emergency, having already caused enormous ill health and mortality worldwide. [1] According to the Joint United Nations Programme on HIV/AIDS (UNAIDS) and WHO reports of November 2010, there are approximately 33.3 million People Living with Human Immunodeficiency Virus/acquired Immunodeficiency Syndrome (HIV/AIDS) (PLWHA) worldwide, with a global prevalence of 0.8%. It is estimated that 90% of the HIV-infected persons live in the developing countries, with the estimated number of infected Indians being 2.31 million and adult prevalence of 0.3%. [2]
HIV/AIDS is no longer just a public health issue in India but become one of the most serious socioeconomic and developmental concerns, because nearly 89% of reported cases are occurring in sexually active and economically productive age group (15-44years). Deaths of young adults have an especially damaging impact on their families and communities, skills are lost, workforce shrinks, and children are orphaned. [3]
From the moment scientists identified HIV/AIDS, social responses of fear, denial, stigma, and discrimination have accompanied the epidemic. Discrimination has spread rapidly, fuelling anxiety and prejudice against the groups most affected as well as those living with HIV/AIDS. It goes without saying that HIV and AIDS are as much a social phenomenon as they are biological and medical concerns. [4]
Hence considering this, the present study conducted to assess the rate of disclosure of HIV serostatus, reactions by the HIV/AIDS patients and their spouse, and discrimination faced by the patients.
Methods
The present cross-sectional study was conducted at antiretroviral therapy (ART) center of a rural tertiary care hospital, situated in Marathawada region of Maharashtra state, from November 2008 to October 2010. The permission from head of institution and clearance from ethics committee was obtained before starting the study. The HIV-positive patients coming to ART center for treatment were included in the study after ensuring confidentiality and obtaining informed consent from them. Patients visiting to "Integrated Counselling and Testing Centre" (ICTC), "Prevention of Parent to Child Transmission" (PPTCT), and admitted in various wards were excluded from the study due to ethical considerations. Children were also not included in the study because it was difficult to assess their psychosocial status. In total, such 801 HIV-positive patients who came to ART center during the study period were studied. These patients were interviewed by the authors itself using a preformed questionnaire. Questions were asked to enquire about sociodemographic characteristics, their immediate reaction after diagnosis, disclosure of serostatus, and discrimination faced by them. The data were analyzed using descriptive statistics and Chi-square test.
Results
In the present study out of 801 patients, the male patients (545, 68.04%) outnumbered the female (256, 31.96%). Maximum number of males (435, 79.81%) and females (217, 84.77%) were in the age group of 20-39 years. Maximum patients (565, 70.53%) were residing in rural area.
Majority of patients harboring HIV infection were laborers (412, 51.44%). Among the 801 patients studied, 565 (70.53%) were married and living with their spouse followed by 136 (16.97%) widows, 32 (4%) widower, 32 (4%) unmarried, 20 (2.5%) divorced, and 16 (2%) separated. Socioeconomic status of the patients revealed 285 (35.58%) and 245 (30.59%) patients from class IV and V socioeconomic status, respectively.
[Table - 1] shows the distribution of HIV-positive patients according to their immediate reactions after diagnosis revealed that the most common reaction after diagnosis was "fear" (593, 74.03%) followed by "depression" (385, 48.06%), "suicidal thoughts" (98, 12.25%). Other reactions were "panic, anger, disgust, and surprise." Hundred (12.48%) patients reported no reaction after diagnosis.
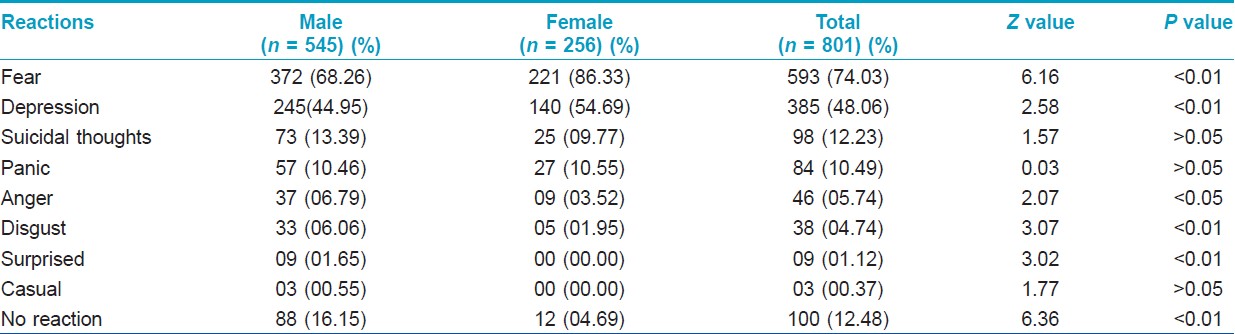
Significantly, fear (221, 86.33%) and depression (140, 54.69%) as an immediate reaction after diagnosis were more in females as compared with males [fear (372, 68.26%), depression (245, 44.95%)] (P<0.01).
More male patients had "suicidal thoughts" (73, 13.48%) and were "panic" (57, 10.46%) as compared with female patients [suicidal thoughts (25, 9.77%), panic (27, 10.55%)] but this difference was not statistically significant (P>0.05). Significantly, more number of male patients (88, 18.15%) did not show any immediate reaction after their diagnosis than female patients (12, 4.69%) (P<0.05).
Out of 801 patients, 769 (96%) had spouse and 32 (4%) male patients were unmarried [Table - 2]. Out of 769, maximum number of patients (653, 84.92%) had disclosed HIV status to their spouses. The disclosure rate was significantly more in females (237, 92.58%) as compared with males (416, 81.09%) (P<0.01).
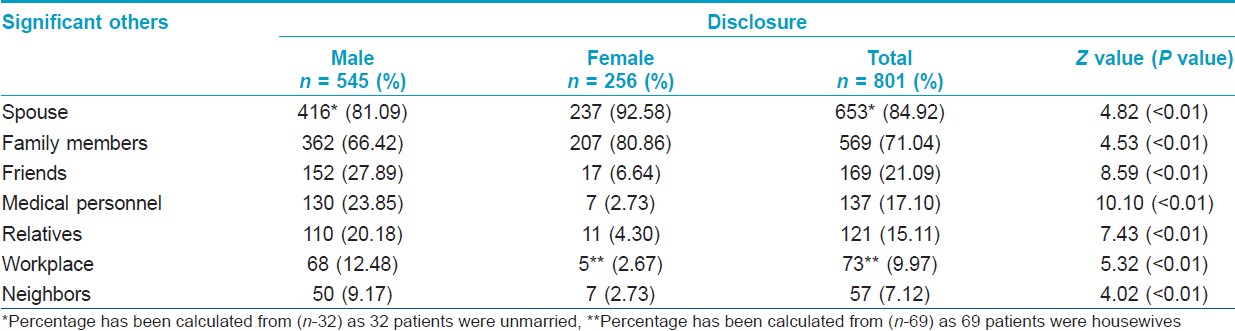
Five hundred and sixty-nine (71.04%) patients had disclosed HIV status to their family members. Significantly, more number of females (207, 80.86%) disclosed HIV status to their family members than males (362,66.42%) (P<0.01). Overall, disclosure rate was very high (789, 98.5%).
[Table - 3] shows the distribution of patients according to immediate reactions of spouse after disclosure of HIV serostatus revealed that among 653 patients who disclosed HIV status to their spouses, wives (spouse of male patient) were 416 (63.71%) and husbands (spouse of female patient) were 237 (36.29%). Majority of spouse (324, 42.13%) had immediate reaction/thought that "their partner had done some crime." The other immediate reactions by spouse were "horror" (294, 38.23%), "anger" (237, 36.29%), and "punishment" (208, 21.045). No reaction was reported by 51 (6.63%).
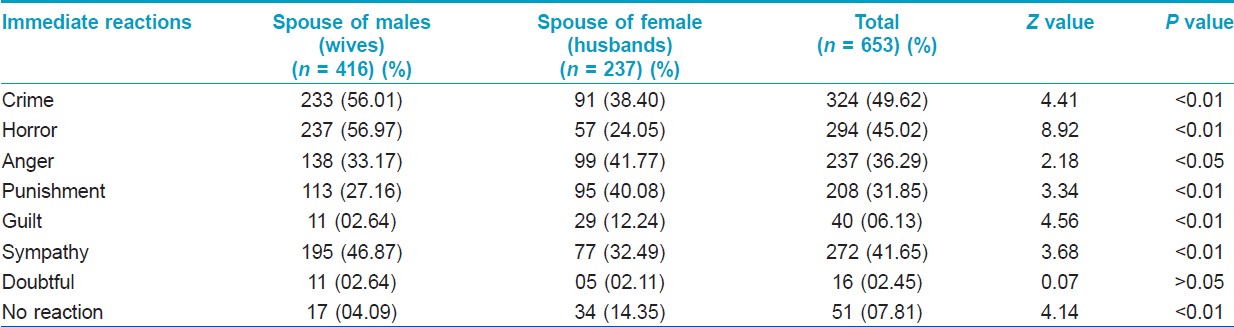
Wives had the "crime" (233, 45.42%) as a predominant immediate reactions after diagnosis as compared to husbands (91, 35.35%) and this difference was found to be statistically significant (P<0.01). Significantly, more percentage of wives expressed "horror" (237, (46.19%) as a immediate reactions after diagnosis as compared to husbands (57, 22.16%) (P<0.01).
More number of husbands showed punishment (95, 37.10%) as immediate reaction to diagnosis compared to wives (113, 22.02%) (P<0.01). Thirty-four (13.28%) husbands did not show any reaction after they came to know about diagnosis of their partner as compared to wives (17,3.31%) (P<0.01).
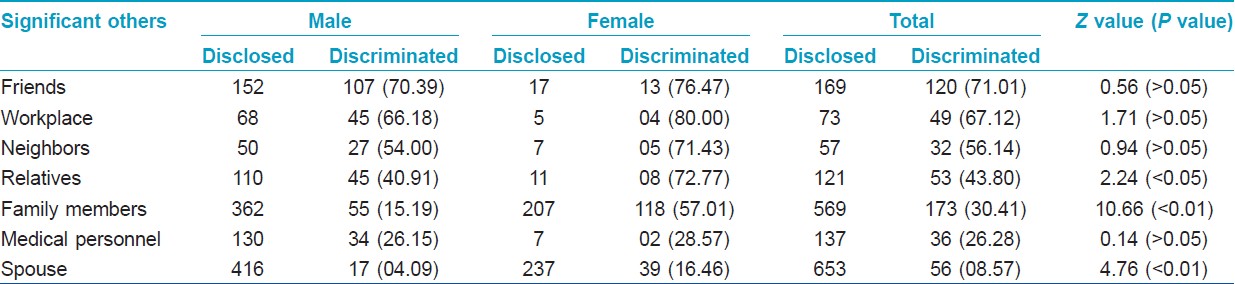
[Table - 4] shows the distribution of patients according to discrimination they faced after disclosure of HIV serostatus showed that maximum number of patients were discriminated by friends (20, 71.01%) followed by discrimination at workplace (49, 67.12%), by neighbors (32, 56.14%), by relatives (53, 43.80%), by family members (173, 30.41%), by medical personnel (36, 26.28%), and by spouse (56, 8.57%). Significantly, more number of females were discriminated by spouse (39, 16.46%), family members (118, 57.01%), and relatives (8, 72.01%) as compared to males [spouse (17, 4.09%), family members (55, 15.19%), and relatives (45, 40.91%)].
Discussion
HIV/AIDS is a potentially sensitive subject and discussion about it can provoke strong reactions from patients. To be diagnosed as HIV-positive patient is traumatic and its natural corollaries are fear, depression, panic, anger, disgust, etc. [5] In this study, the foremost reaction of patients after coming to know about their seropositivity was fear (593, 74.03%) which primarily manifested as fear of future, fear of death, fear of marital disharmony, fear of being avoided, etc. These fears are also reported by Muley [5] as a reason for non-disclosure of seropositive status. This may be related to the fact that till date there is no effective cure. Discrimination and stigmatization of PLWHA by society at various levels might also contribute to these various fears.
The second most common reaction of HIV-positive patients was depression (385, 48.06%). "Depression" was also reported by Chandra et al. [6] (40%) and Melanie et al. [7] (46.85%).
The reaction of fear (221, 86.33%) and depression (140, 54.69%) was significantly more common in females than males [fear (372, 68.26%), depression (245, 44.95%)] (P<0.01). Males in our society are considered independent. They are generally economically self-sufficient, whereas females even if economically self-sufficient are dependant. This may explain more fear in females.
Ninety-eight (12.23%) patients had thought of ending their life even before disease could actually kill them. Suicidal thoughts among these patients might have originated because of fear and devastating effects of stigma and discrimination prevalent in the society. Suicidal thoughts as a reaction after dignosis were also quoted by Kalichman et al.[8] (26%) and Chandra et al.[6] (24%), respectively.
Human immunodeficiency virus status disclosure to significant others
overwhelming majority of patients did not want to reveal their Human immunodeficiency virus (HIV) status to anyone other than spouse and family members. Majority of patients had disclosed HIV status to their spouses (653, 84.92%) and family members (569, 71.04%). Among those who disclosed their serostatus to spouse and family members, females [spouse (237, 92.58%), family members (207, 80.86%)] were significantly more than males [spouse (416, 81.09%), family members (362, 66.42%)] (P<0.01).
High disclosure rate of HIV serostatus to the spouse/partner was also reported by Bouillon et al. [9] (84.6%) and Muley [5] (62%). Likewise, higher disclosure rate to family members (37.2%, 78%) was also reported by Muley [5] and Chandra et al.[6]
The reason for disclosure to spouse or family members is obvious. For couples, spouse/partner is the first and the most reliable and confident person. Disclosure of HIV status to one′s sexual partner is an important prevention goal emphasized by WHO and Centre for disease control and prevention (CDC) in their protocols for HIV counseling and testing. [10] However, the reason for disclosing to family members may be due to the fact that they were the primary care takers of patients and could give emotional and financial support to patients.
One hundred and sixty-nine (21.09%) patients had disclosed their HIV status to friends and 121 (15.11%) to relatives. Similar to present study, low disclosure to friends and relatives was also quoted by Chandra et al. [6] (friends, 7%), Bouillon [9] (friends and relatives, 55.6%), and Muley [5] (friends, 20.95; relatives, 30.2%).
This disclosure is well-observed phenomenon with behavioral practices of HIV patients. This could be for emotional support and the need to share feelings with them. Disclosure to relatives could be for financial support and need to prevent marriage plans.
One hundred and thirty-seven (17.10%) patients had revealed their status to their doctors. Similarly, 15% patients disclosed their HIV status to health professionals in a study by Chandra et al. [6] However, in contrast with the present study, 62% of patients disclosed their HIV status to doctors in a study by Muley. [5] The obvious reason could be need for treatment.
Twelve (1.49%) patients had not disclosed their serostatus in anticipation of negative social reasons, fear of internalization of stigma and discrimination, and disgrace to family. This may lead to late diagnosis.
Immediate reactions of spouse after disclosure
More number of husbands (spouse of female) revealed "punishment" (37.10%) as immediate reaction to disclosure, 32.03% of husbands expressed that they had a "verbal fight" with their spouse, and wives (spouse of male) showed "crime" (45.42%) and "horror" (46.19%) as a predominant immediate reactions after disclosure.
The reaction of "guilt" shown by husbands (12.24%) on knowing the seropositive status of wives indicates that they held themselves responsible for seropositive status of spouse. If the husbands develop an attitude of "being responsible for health of their spouse" especially in case of HIV/AIDS then that would definitely help to reduce the HIV/AIDS problem. Interestingly, 195 (46.87%) wives and 77 (32.49%) husbands showed sympathetic reactions to their spouses. Such an attitude may help themselves to come in terms with reality and care each other. The reaction to disclosure may be originating from the importance given to sex to outside marriage in our community.
In this study, majority of females were illiterate and from lower socioeconomic class. Because of the sociocultural set up, females keep immense faith in their spouses (husbands). So rightfully, majority of the wives had negative reactions such as feeling of crime (233, 56.01%) committed by husband, anger (138, 33.17%) toward husband, etc. Wives (spouse of male) were horrified (237, 56.97%) after knowing the diagnosis of their husbands. They were concerned about the effect of this on their livelihood and the chances of transmission of disease to themselves.
Discrimination of patients after disclosure
related prejudice and discrimination directed at PLWHA, groups and communities to which they belong is a worldwide phenomenon. [4] In this study, maximum number of patients were discriminated by friends (120, 71.01%). Lack of awareness about the disease and fear of contracting it from the patient could have been the reason for discrimination. In contrast to this study, Patrick, et al. [11] reported discrimination of 12% patients by friends.
About 67.12% of patients were discriminated at workplace. Although HIV is not transmitted in the majority of workplace settings, the supposed risk of transmission has been used by numerous employers to terminate or refuse employment. In contrast to this study, discrimination of 7.1%and 5.71% patients at workplace quoted by Peretti-Watel et al., [11],[ 12] respectively.
One hundred and seventy-three (30.41%) patients reported discrimination by family members. Significantly, more number of females (118, 57.01%) were discriminated by family members as compared with males (55, 15.19%) (P<0.01). In the majority of developing countries, families are the primary care givers to sick members. There is clear evidence of the importance of the role that the family plays in providing support and care for PLWHA.
However, not all family response is positive. Infected members of the family can find themselves stigmatized and discriminated against within the home. [10] However, findings quoted by Taraphdar, et al. [10] (12.5%) and Sharma, et al. [12] (8.57%) regarding discrimination by family members were not in accordance with this study.
Thirty-six (26.28%) patients experienced discrimination by medical personnel. Lack of protective and other material needed to treat and prevent the spread of HIV might have contributed to discriminatory behavior. It is unfortunate that the very same people engaged in helping these people indulge in discriminatory behavior. Similar findings (27%) (14.29%) with the present study were observed by. [11],[12]
Least number of patients were discriminated by their spouse (56,8.57%). Discrimination of 14.29% patients by spouse was reported by. [12]
In this study, discrimination was directed more toward female patients by all groups. Even a married woman who has been infected by her husband will be accused by her in-laws. In such a male-dominated society, no-one ever accepts that the man is actually the one who did something wrong. It is even harder on unmarried women since it is seen as a fair result of their sexual misbehavior.
| 1. |
Narain JP. AIDS in Asia, The Challenge Ahead. New Delhi: WHO, Regional Office SEAR; 2004. p. 15-9.
[Google Scholar]
|
| 2. |
WHO/UNAIDS. AIDS Epidemic Update, 2010. Available from: http://www.unaids.org/en/HIV-data Last accessed on 2010 Feb 12.
[Google Scholar]
|
| 3. |
Kishore. National Health Programmes of India. 6 th ed. New Delhi: Century Publications; 2006. p. 138.
[Google Scholar]
|
| 4. |
HIV/AIDS stigma and discrimination, 2007. Available from: http://www.avert.org Last accessed on 2008 Nov 3.
[Google Scholar]
|
| 5. |
Muley R. Confidentiality, stigma, discrimination and voluntary disclosure. Indian J Soc Work 2005;66:310-21.
[Google Scholar]
|
| 6. |
Chandra PS, Deepthivarma S, Manjula V. Disclosure of HIV infection in south India: Patterns, reasons and reactions. AIDS Care 2003;15:207-15.
[Google Scholar]
|
| 7. |
Rusch M, Nixon S, Schilder A, Braitstein P, Chan K, Hogg RS. Impairments, activity limitations and participation restrictions: Prevalence and associations among persons living with HIV/AIDS in British Columbia. Health Qual Life Outcomes 2004;2:46.
[Google Scholar]
|
| 8. |
Kalichman SC, Heckman T, Kochman A, Sikkema K, Bergholte J. Depression and thoughts of suicide among middle-aged and older persons living with HIV-AIDS. Psychiatr Serv 2000;51:903-7.
[Google Scholar]
|
| 9. |
Bouillon K, Lert F, Sitta R, Schmaus A, Spire B, Dray-Spira R. Factors correlated with disclosure of HIV infection in the French Antilles and French Guiana: Results from the ANRS-EN13-VESPA-DFA Study. AIDS 2007;21 Suppl 1:S89-94.
[Google Scholar]
|
| 10. |
Taraphdar P, Dasgupta A, Saha B. Disclosure among people living with HIV/AIDS. Indian J Community Med 2007;32:280-2.
[Google Scholar]
|
| 11. |
Peretti-Watel P, Spire B, Obadia Y, Moatti JP, VESPA Group. Discrimination against HIV-infected people and the spread of HIV: Some evidence from France. PLoS One 2007;2:e411.
[Google Scholar]
|
| 12. |
Sharma A, Shah S, Marfatia YS. Discrimination faced by HIV positive females. Indian J Sex Transm Dis 2005;26:70-1.
[Google Scholar]
|
Fulltext Views
1,848
PDF downloads
1,346





![[Table - 1]](#tbl_ijdvl_2013_79_1_135_104690_t1.jpg){kind=link}
![[Table - 2]](#tbl_ijdvl_2013_79_1_135_104690_t2.jpg){kind=link}
![[Table - 3]](#tbl_ijdvl_2013_79_1_135_104690_t3.jpg){kind=link}
![[Table - 4]](#tbl_ijdvl_2013_79_1_135_104690_t4.jpg){kind=link}