Translate this page into:
Hyperhidrosis, vesicles, and papules over the nose: Granulosis rubra nasi
Correspondence Address:
Sidharth Sonthalia
C-122, Sushant Apartments, Sushant Lok-1, Block-C, Gurgaon 122 001
India
| How to cite this article: Sonthalia S, Singal A, Sharma R. Hyperhidrosis, vesicles, and papules over the nose: Granulosis rubra nasi. Indian J Dermatol Venereol Leprol 2012;78:97-98 |
A 16-year-old boy presented with multiple erythematous lesions over the nose and cheeks along with minimal itching for 5 years. Lesions started with the development of excessive sweating over the tip of nose that extended to involve the central face, followed by the gradual appearance of diffuse redness over the nose and cheeks. There was no history suggestive of hyperhidrosis of palms and soles, photosensitivity, or poor peripheral circulation. Family history was insignificant. Physical examination revealed hyperhidrosis and erythema over the centrofacial region along with multiple 1-3-mm-sized erythematous papules and vesicles over the dorsum, tip and alae of nose, adjoining areas of the cheeks, glabella, and philtrum [Figure - 1]. Rest of the physical examination was normal. Lesional skin biopsy showed epidermal thinning and vascular dilatation of upper and mid-dermal blood vessels and perivascular lymphohistiocytic infiltrate [Figure - 2]. The patient was counseled about the benign and self-limiting nature of the disease.
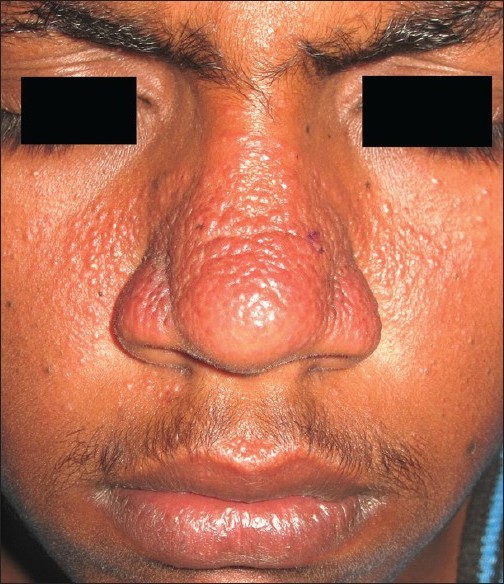 |
| Figure 1: Erythematous papulovesicular lesions overlying a background of diffuse erythema and hyperhidrosis on the dorsum and alae of the nose, cheeks, glabella, and philtrum |
 |
| Figure 2: Prominent vascular dilatation with perivascular lymphohistiocytic infiltrate in the mid-dermis (H and E, ×400) |
First described by Jadassohn in 1901, granulosis rubra nasi (GRN) is a rare disease of the eccrine glands. It generally appears during early childhood, but adolescent and adult onset is possible. The initial symptom of hyperhidrosis of the central face, most conspicuously on the tip of nose, may be present for years before the development of characteristic erythema over nose, cheeks, chin, and upper lip. The erythema is covered by sweat droplets; papules, vesicles, and small cysts may form at eccrine orifices. The condition is mostly asymptomatic except for mild pruritus. Primary concerns of the patients are cosmetic and hyperhidrosis, which tend to worsen in summer. Association with primary palmoplantar hyperhidrosis, acrocyanosis, and poor peripheral circulation has been observed. Granulosis rubra nasi usually resolves spontaneously around puberty, though it may persist indefinitely with conspicuous telangiectasia and cystic lesions. Heid et al. reported GRN with pheochromocytoma in a 19-year-old woman, in whom surgical removal of the tumor led to involution of the hyperhidrosis and regression of the nasal dermatosis.
The diagnosis of GRN is primarily clinical owing to its distinctive morphology. Clinical differential diagnoses include eccrine hidrocystoma and inflammatory or photosensitive dermatoses such as rosacea, perioral dermatitis, and lupus erythematosus. Multiple eccrine hidrocystoma of the Robinson-type simulate GRN clinically with the presence of multiple translucent, dome-shaped papules on the periorbital and malar areas with the frequent presence of craniofacial hyperhidrosis. However, the onset of lesions is later (typically seen in middle-aged females) and the facial erythema characteristic of GRN does not occur. Persistent erythema of the central face is seen in both GRN and rosacea. However, the latter is also characterized by a later age of onset and the presence of vasomotor symptoms such as flushing. Perioral dermatitis presents with discrete papules, vesicles, and pustules (often with a background of erythema and scaling) typically distributed over perioral and sometimes perinasal and periorbital regions. The photosensitive malar rash of lupus erythematosus consists of confluent symmetric erythema and edema with no vesiculation, over malar eminences, and nasal bridge with sparing of nasolabial folds. None of these conditions show hyperhidrosis of the central face - the most important and constant feature of GRN. Histopathology easily differentiates the above conditions from GRN.
On histopathology, dilated dermal blood vessels and lymphatics with perivascular mononuclear infiltration are seen. These changes are often accompanied by cystic dilatation of eccrine ducts, at times simulating a hidrocystoma. Eccrine hidrocystoma also shows solitary or multiple cysts lined by a double layer of cuboidal cells on histology, but dilatation of dermal vessels and perivascular mononuclear infiltrate is not seen.
The pathogenesis of GRN remains obscure. It is likely to represent a unique form of sweat retention with the occurrence of erythema, papules, and vesiculation as secondary changes. Familial cases have been reported, and both autosomal dominant and recessive modes of inheritance have been suggested.
Counseling the patients about the self-limiting nature of the condition is most important. Therapies such as topical indomethacin, oral corticosteroid, tetracycline, and cryotherapy have resulted in only modest and temporary benefit. Recently, the symptoms of GRN in a 16-year-old boy significantly improved following a single injection of botulinum toxin type A. Although hyperhidrosis recurred within a year of treatment, botulinum toxin may be considered an effective therapeutic option.
Fulltext Views
6,410
PDF downloads
3,299





![[Figure - 1]](#fig_ijdvl_2012_78_1_97_90957_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2012_78_1_97_90957_f2.jpg){kind=link}