Translate this page into:
Hyperpigmentation along Blaschko lines
2 Department of Pathology, Maulana Azad Medical College, New Delhi, India
Correspondence Address:
Sumit Sethi
Department of Dermatology, Maulana Azad Medical College, Bahadur Shah Zafar Marg, New Delhi - 110 002
India
| How to cite this article: Barman KD, Sethi S, Garg VK, Khurana N. Hyperpigmentation along Blaschko lines. Indian J Dermatol Venereol Leprol 2015;81:66-68 |
Sir,
The lines of Blaschko represent the routes of ectodermal cell migration from the neural crest. Various inherited and acquired disorders of hyperpigmentation have been described along these lines. Different descriptive terms for these disorders include "linear and whorled nevoid hypermelanosis" (LWNH), [1] "progressive cribriform and zosteriform hyperpigmentation" (PCZH), [2] "zebra-like hyperpigmentation in whorls and streaks," [3] and "reticulate hyperpigmentation in a zosteriform pattern." [4] These designations do not encompass the entire spectrum of clinical manifestations and therefore these pigmentary anomalies need to be reclassified along with other mosaic disorders.
An 18-year-old male presented to the dermatology outpatient clinic of Lok Nayak Hospital with asymptomatic patchy hyperpigmentation on his torso and right upper limb. Uniformly pigmented, dark brown macules of size 0.1-1 cm, with irregular and well defined margins, were arranged linearly, along the lines of Blaschko, from the xiphi-sternum to the palmar aspect of the right thumb in an inverted U pattern, forming an arc on the upper chest and a V pattern on the back. [Figure - 1] and [Figure - 2]. His face, mucosae, eyes, hair, teeth and nails were spared and systemic examination was within normal limits. The skin lesions had initially appeared a year ago on the volar aspect of his forearm and gradually progressed to their present extent over a period of 6 months. For the past 6 months, there had been no change in the number, size or color of macules. There was no history suggestive of preceding inflammation, blisters, or verrucous lesions. His growth and development had been normal and family history was not contributory.
 |
| Figure 1: Uniformly pigmented dark brown macules in a linear distribution along the lines of Blaschko, extending from the xiphi-sternum to palmar aspect of the right thumb in an inverted U pattern and forming an arc on upper chest |
 |
| Figure 2: Dark brown macules forming a V pattern on back |
Histopathology revealed increased melanization of the basal layer with patchy small foci of normal basal layer pigmentation, in the absence of dermal melanophages and pigment incontinence [Figure - 3].
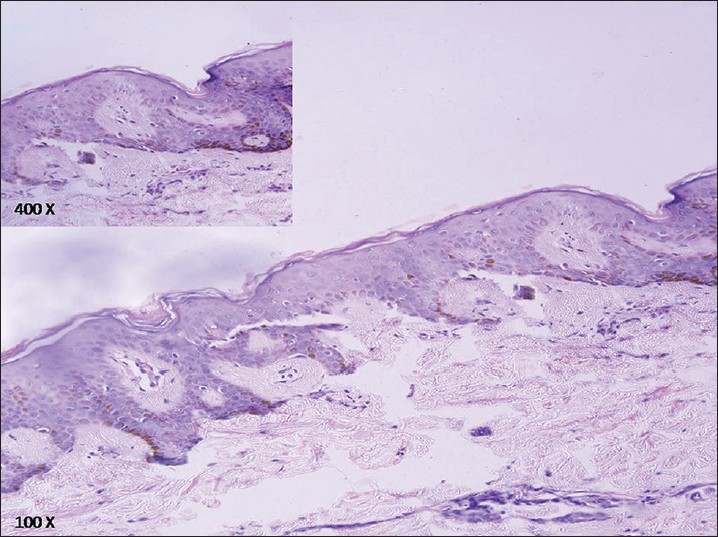 |
| Figure 3: Increased melanization of the basal layer without evidence of dermal melanophages or pigment incontinence (H and E: ×100). There were large areas of hyperpigmentation interspersed with patchy small foci of normal basal layer pigmentation. Inset (×400) |
Mosaicism, leading to the proliferation and migration of two mixed populations of melanocytes with different potential for pigment production, is the most likely cause of pigmentary disorders along the lines of Blaschko. Inherited and/or nevoid disorders of hyperpigmentation that follow these lines include LWNH, third stage of incontinentia pigmenti, and early stage of epidermal nevus. Acquired mosaic pigmentary conditions include hyperpigmentation secondary to linear lichen planus (pigmentosus) and linear fixed drug eruption. [1],[2]
Linear and whorled nevoid hypermelanosis was first defined by Kalter et al.[1] in 1988 as a sporadic pigmentary anomaly occurring within the first few weeks of birth, characterized clinically by swirls and streaks of macular hyperpigmentation along the lines of Blaschko and histologically by epidermal melanosis without pigment incontinence. It tends to spare the mucous membranes, eyes, palms, and soles, and has a possible association with congenital anomalies. Zebra-like hyperpigmentation described by Alimurung [3] was probably the same clinical entity, although described in a dermatomal distribution.
Progressive cribriform and zosteriform hyperpigmentation was first described by Rower et al. as uniformly tan cribriform macular pigmentation in a zosteriform distribution, with no evidence of preceding inflammation, and histologically characterized by basal layer hypermelanosis. It has an onset well after birth and lacks any associated cutaneous or systemic abnormalities. [2] In terms of clinical features, "reticulate hyperpigmentation in a zosteriform pattern" described by Iijima closely resembled the former. [4]
The existence of a plethora of terms for such pigmentary disorders leads to a lot of confusion. On careful scrutiny, the cases of progressive cribriform and zosteriform hyperpigmentation described by Cho et al.[5] and Schepis et al., [6] had pigmentation along the lines of Blaschko rather than in a zosteriform distribution. " Reticulate hyperpigmentation in a zosteriform pattern" reported by Iijima in children, involved multiple dermatomes and additionally, involved Blaschko and Voigt′s lines as well. [4] However, in the original account of progressive cribriform and zosteriform hyperpigmentation by Rower et al., [2] the lesions were limited to only one quadrant of the body and the age of onset was in adolescence.
A solution to this problem has been proposed by different authors in the past. Quecedo et al. recommended the unification of all these anomalies of hyperpigmentation under the name "Linear and whorled nevoid hypermelanosis." [7] Some regard them as a heterogeneous continuum of pigmentary mosaicism with progressive cribriform and zosteriform hyperpigmentation at one end and linear and whorled nevoid hypermelanosis at the other, [5],[8] while others have hypothesized that progressive cribriform and zosteriform hyperpigmentation is the late onset variant of linear and whorled nevoid hypermelanosis, which can be associated with systemic involvement. [6] Nehal et al.[8] have advocated using descriptive terms such as "hyperpigmentation and/or hypopigmentation along the lines of Blaschko" when evaluating such patients while Taibjee et al.[9] have advised an umbrella term "pigmentary mosaicism."
Pigmentation in our case, was linear without the formation of whorls or streaks, and extended to involve the palmar surface of the right hand. The eruption was bilateral, asymmetric, and differed from the widespread involvement of linear and whorled nevoid hypermelanosis and also from the unilateral zosteriform involvement in progressive cribriform and zosteriform hyperpigmentation. It manifested as a purely cutaneous eruption without any systemic involvement. A diffuse or localized pattern, association with congenital anomalies and age of onset are the key features differentiating the above entities. The features seen in our patient with Blaschkoid hypermelanosis probably fit somewhere in the clinical spectrum of zosteriform and naevoid whorled hypermelanoses, and cannot be exactly designated using the available terminology. Older terms like linear and whorled nevoid hypermelanosis and progressive cribriform and zosteriform hyperpigmentation do not sufficiently encompass the entire range of clinical manifestations and lead to a lot of misunderstanding regarding these mosaic pigmentary disorders. These confusing terms should be discarded; a revised nomenclature and classification of these pigmentary anomalies is the need of the hour.
| 1. |
Kalter DC, Griffiths WA, Atherton DJ. Linear and whorled nevoid hypermelanosis. J Am Acad Dermatol 1988;19:1037-44.
[Google Scholar]
|
| 2. |
Rower JM, Carr RD, Lowney ED. Progressive cribriform and zosteriform hyperpigmentation. Arch Dermatol 1978;114:98-9.
[Google Scholar]
|
| 3. |
Alimurung FM, Lapenas D, Willis I, Lang P. Zebra-like hyperpigmentation in an infant with multiple congenital defects. Arch Dermatol 1979;115:878-81.
[Google Scholar]
|
| 4. |
Iijima S, Naito Y, Naito S, Uyeno K. Reticulate hyperpigmentation distributed in a zosteriform fashion: A new clinical type of hyperpigmentation. Br J Dermatol 1987;117:503-10.
[Google Scholar]
|
| 5. |
Cho E, Cho SH, Lee JD. Progressive cribriform and zosteriform hyperpigmentation: A clinicopathologic study. Int J Dermatol 2012;51:399-405.
[Google Scholar]
|
| 6. |
Schepis C, Alberti A, Siragusa M, Romano C. Progressive cribriform and zosteriform hyperpigmentation: The late-onset feature of linear and whorled nevoid hypermelanosis associated with congenital neurological, skeletal and cutaneous anomalies. Dermatology 1999;199:72-3.
[Google Scholar]
|
| 7. |
Quecedo E, Febrer I, Aliaga A. Linear and whorled nevoid hypermelanosis. A spectrum of pigmentary disorders. Pediatr Dermatol 1997;14:247-8.
[Google Scholar]
|
| 8. |
Nehal KS, PeBenito R, Orlow SJ. Analysis of 54 cases of hypopigmentation and hyperpigmentation along lines of Blaschko. Ach Dermatol 1996;132:1167-70.
[Google Scholar]
|
| 9. |
Taibjee SM, Bennett DC, Moss C. Abnormal pigmentation in hypomelanosis of Ito and pigmentary mosaicism: The role of pigmentary genes. Br J Dermatol 2004;151:269-82.
[Google Scholar]
|
Fulltext Views
13,849
PDF downloads
3,666





![[Figure - 1]](#fig_ijdvl_2015_81_1_66_148580_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2015_81_1_66_148580_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2015_81_1_66_148580_f3.jpg){kind=link}