Translate this page into:
Hypohidrotic ectodermal dysplasia in association with milia
Correspondence Address:
Sharad Mehta
R/0 8A, Tulsi Nagar, Hiran Magri Sector 5, Udaipur - 313 001, Rajasthan
India
| How to cite this article: Mehta S, Agarwal N, Khare AK, Kuldeep C, Mittal A, Gupta LK. Hypohidrotic ectodermal dysplasia in association with milia . Indian J Dermatol Venereol Leprol 2014;80:483 |
Sir,
Ectodermal dysplasias are a group of inherited disorders that share in common developmental defects involving structures derived from the ectoderm. They are broadly classified into hypohidrotic/anhidrotic and hidrotic ectodermal dysplasias on the basis of presence or absence of sweating. Anhidrotic/hypohidrotic ectodermal dysplasia can be inherited as an X-linked, autosomal dominant or autosomal recessive disorder. Hypohidrotic ectodermal dysplasia is the most common of the ectodermal dysplasias and is characterized by hypotrichosis, hypodontia, hypohidrosis, and distinctive facial features such as frontal bossing, depressed mid-face, saddle nose, and full everted lips. It is caused by mutations involving the gene ectodysplasin which plays a critical role in the morphogenesis of teeth, hair, and sweat glands. Milia are superficial, white globoid lesions, 1-2 mm in diameter usually occurring spontaneously on the face in predisposed individuals. They are derived from the lowest portion of the infundibulum of vellus hair at about the level of the sebaceous duct. The body of the white milium is made up of laminated keratin. Milia-like eruptions on face, though rare, have been reported in patients of hypohidrotic ectodermal dysplasia in the past.
A 19-year-old male presented to us with small, cream-colored, milia-like, discrete but aggregated, variably sized papular eruptions over almost the entire face with sparing of periocular and perioral areas [Figure - 1]. The lesions developed gradually at the age of 12 years and progressed over a period of 3 years. No similar lesions were noted elsewhere on the body. The patient had a distinct facies with a prominent forehead, periorbital wrinkling and hyperpigmentation, depressed mid-face, and full everted lips. Only five peg-shaped upper teeth were present. Body hair were sparse. The patient had history of intolerance to hot environments since childhood. The history of scaling or collodion membrane at birth could not be elicited. None of the family members had any similar complaints. Starch iodine test revealed marked hypohidrosis of palms. The above features led us to make a clinical diagnosis of hypohidrotic ectodermal dysplasia, probably due to a sporadic mutation. The skin biopsy showed a small, milia-like cyst lined by keratinized stratified squamous epithelium [Figure - 2]. No sebaceous gland hyperplasia was seen.
 |
| Figure 1: Milia-like papules over face |
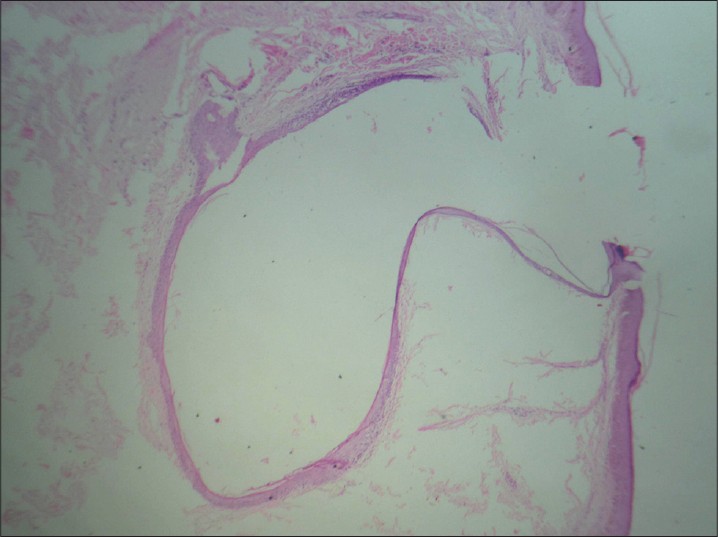 |
| Figure 2: Hematoxylin and eosin (H and E) staining, ×10, showing cyst lined by epidermis |
Milia-like sebaceous facial papules in hypohidrotic ectodermal dysplasia have been described in previous reports by different names: milia, adenoma sebaceum, sebaceous cyst, nevi, and degenerated sebaceous gland with hyperkeratosis. [1],[2],[3] They have been suspected to be due to a missense mutation in the tumor necrosis factor-like domain in ectodysplasin A. [4] Varied histopathological findings have been described in biopsies from these lesions. [2],[4] Most reports attribute the origin of the milia-like papules to large, sebaceous glands. The origin of these lesions has also been attributed to eruptive vellus hair cysts. [5] In our case, we found an epidermoid cyst without any sebaceous gland hyperplasia. The keratin in the cyst might have been lost during processing of the specimen for histopathology. Ectodermal dysplasias affect the differentiation of ectodermally-derived structures resulting in a wide variety of phenotypes. This probably results from various missense mutations in the ED1 gene. Milia-like lesions appear to be present in a small minority of patients with hypohidrotic ectodermal dysplasia, and that too, mainly in males. [2],[4] In addition, they have been found to develop after puberty. [4] This has been explained in the past by the intact sexual maturation in these patients leading to androgen secretion at puberty which exerts an effect on the partially defective pilosebaceous units. Our finding of milia might also be a part of this phenotypic spectrum.
| 1. |
Goeckermann WH. Congenital ectodermal defect: With report of a case. Arch Dermatol Syph 1920; 1:396-412.
[Google Scholar]
|
| 2. |
Katz SI, Penneys NS. Sebaceous gland papules in anhidrotic ectodermal dysplasia. Arch Dermatol 1971; 103:507-9.
[Google Scholar]
|
| 3. |
Orge C, Bonsmann G, Hamm H. Multiple sebaceous gland hyperplasias in X chromosome hypohidrotic ectodermal dysplasia. Hautarzt 1991; 42:645-7.
[Google Scholar]
|
| 4. |
Hsu MM, Chao SC, Lu AC. A novel missense mutation (Gln306His) in exon 7 of the ED1 gene causing anhidrotic ectodermal dysplasia with prominent milia-like facial sebaceous papules. Br J Dermatol 2003; 149:443-5.
[Google Scholar]
|
| 5. |
Köse O, Taºtan HB, Deveci S, Gür AR. Anhidrotic ectodermal dysplasia with eruptive vellus hair cysts. Int J Dermatol 2001; 40:401-2.
[Google Scholar]
|
Fulltext Views
4,386
PDF downloads
2,679





![[Figure - 1]](#fig_ijdvl_2014_80_5_483_140348_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2014_80_5_483_140348_f2.jpg){kind=link}