Translate this page into:
Idiopathic CD4 lymphocytopenia presenting as recurrent giant molluscum contagiosum
2 Department of Skin, Primus Super Specialty Hospital, Chankyapuri, New Delhi, India
3 Department of Pathology, Army College of Medical Sciences and Base Hospital, Delhi Cantt, New Delhi, India
Correspondence Address:
Sandeep Arora
Skin Department, Army College of Medical Sciences and Base Hospital, Delhi Cantt, New Delhi - 110 010
India
| How to cite this article: Arora S, Arora G, Sahai K, Borde P. Idiopathic CD4 lymphocytopenia presenting as recurrent giant molluscum contagiosum. Indian J Dermatol Venereol Leprol 2013;79:555 |
CD4 lymphocytopenia is well known in HIV infection and disorders of immunodeficiency and may occur as a transitory phenomenon under immunosuppressive medication or viral infections. [1] Idiopathic CD4 lymphocytopenia (ICL) was initially described by the Center for Disease Control and Prevention (CDC) [2]
in 1992 and has been rarely reported in literature thereafter. [3]
A 60-year-old male presented with recurrent large painless, nodular lesions of 8 months duration over both upper and lower extremities [Figure - 1]. He gave history of repeated recurrences after local management, at our skin center. There was no history of similar complaints. He, however, volunteered history of recurrent furunculosis for the past few years and history of disseminated tuberculosis 6 years back. He was treated adequately with antituberculous therapy and had been followed up thereafter with no evidence of recurrence. There was no history of chronic cough, diarrhoea, weight loss, high risk behaviour, surgeries, or receipt of blood transfusion. He was not on any long-term medications.
 |
| Figure 1: Giant molluscum contagiosum over arm |
On examination, the lesions appeared umbilicated to pearly white on normal skin, while some were inflammed [Figure - 1].
Investigations revealed a normal hemogram, biochemical, and blood sugar profile. Enzyme-linked immunosorbent assay for HIV was repeatedly negative over an 8-month period. Western blot test was also negative. CD4+ T cell count done repeatedly 6 weeks apart revealed consistent low values of 267, 276, 266/ mm 3 . with CD8+T cell count of 378, 271, and 280/mm 3 , respectively. Skin biopsy revealed large ellipsoid, homogeneous, acidophilic cytoplasmic inclusions consistent with molluscum contagiosum [Figure - 2].
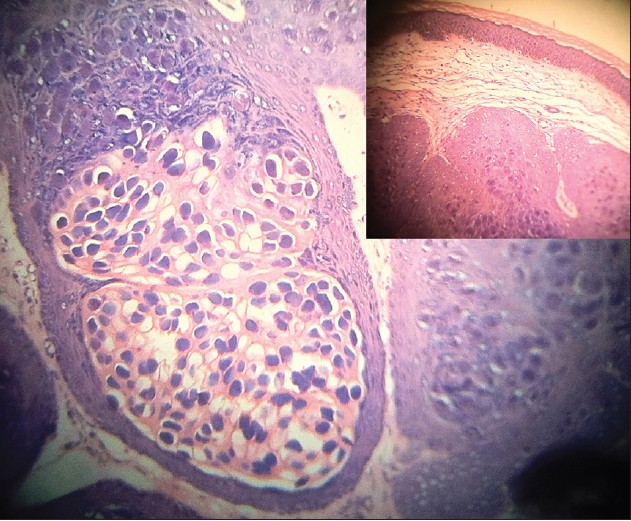 |
| Figure 2: Photomicrograph showing large ellipsoid, homogeneous, and acidophilic cytoplasmic inclusions consistent with molluscum contagiosum (H and E, ×40) with inset (H and E, ×10) |
The patient was investigated to rule out concomitant immune suppressive diseases. Repeated hemogram, biochemical profile, blood sugar profile, and peripheral blood smear were normal. Stool examination was negative for occult blood. Antinuclear antibody and anticardiolipin antibody were negative, thyroid function tests, immunoglobulin profile, and complement levels were within normal limits. Markers for chronic hepatitis B and C were negative.
The patient was diagnosed as a case of idiopathic CD4+ T cell lymphocytopenia. He was managed for his primary complaint of giant molluscum contagiosum with repeated enucleation. He has been observed thereafter over a 6-month period with no evidence of recurrence.
ICL is rare disorder defined by the Center for Disease and Control as follows:
- Decreased number of circulating CD4+T cell lymphocytes (<300 cell/ mm 3 or < 20% of total T cells) on more than one occasion.
- No laboratory evidence of infection with HIV Type I or II.
- Absence of any defined immunodeficiencies or therapy associated with depressed levels of CD4+T cells.
The incidence of CD4+ T cell lymphocytopenia (transient of unknown cause as well as ICL) has been reported as 0.25%-0.5%. [4] Infections most notably HIV infection, malignancies, medications, and autoimmune disorders have been associated with CD4 cell lymphocytopenia. [5] As compared to those with HIV infection, the CD8+ T cell count is not elevated and the immunoglobulin levels are either normal or depressed where as they may be elevated in HIV positive. Our patient had a normal immunoglobulin and complement levels. This disorder is usually diagnosed after an opportunistic infection or an accidental laboratory finding. The opportunistic infections observed in ICL are similar to those seen in patients with HIV infection. [5] Management of a patient with transient CD4 lymphocytopenia is primarily aimed at the treatment of the underlying cause along with the infection. Management of ICL patients is primarily aimed at the treatment of the opportunistic infection along with chemoprophylaxis of opportunistic infections if the CD4 cell count is less than 200/mm 3 . Measures to improve the CD4+ T cell count include systemic interferon, [3] IL2 therapy; [6] however, the long-term effects are still uncertain. Bone marrow transplantation has been suggested as a cure.
Our patient, a 60-year-old otherwise healthy male, satisfied the above case definition of ICL as he had persistently depressed CD4+ T cell count in the absence of HIV infection. There was no history of high-risk behavior, receipt of any blood transfusions, or surgeries. Immune suppressive disorders such as diabetes, malignancies, and immune suppressive drug intake were ruled out. He has been placed on regular follow-up with an advice for 6-monthly review of his CD4 cell count.
| 1. |
Zonios DI, Falloon J, Bennett JE, Shaw PA, Chaitt D, Baseler MW, et al. Idiopathic CD4+ lymphocytopenia: Natural history and prognostic factors. Blood 2008;112:287-94.
[Google Scholar]
|
| 2. |
Centers for Disease Control (CDC). Unexplained CD4 T-lymphocyte depletion in persons without evident HIV infection-United States. MMWR Morb Mortal Wkly Rep 1992;41:541-5.
[Google Scholar]
|
| 3. |
Böhm M, Luger TA, Bonsmann G. Disseminated giant molluscum contagiosum in a patient with idiopathic CD4+ lymphocytopenia. Successful eradication with systemic interferon. Dermatology 2008;217:196-8.
[Google Scholar]
|
| 4. |
Busch MP, Valinsky JE, Paglieroni T, Prince HE, Crutcher GJ, Gjerset GF, et al. Screening of blood donors for idiopathic CD4+ T-lymphocytopenia. Transfusion 1994;34:192-7.
[Google Scholar]
|
| 5. |
Walker UA, Warnatz K. Idiopathic CD4 lymphocytopenia. Curr Opin Rheumatol 2006;18:389-95.
[Google Scholar]
|
| 6. |
Cunningham-Rundles C, Murray HW, Smith JP. Treatment of idiopathic CD4 T lymphocytopenia with IL-2. Clin Exp Immunol 1999;116:322-5.
[Google Scholar]
|
Fulltext Views
1,697
PDF downloads
1,504





![[Figure - 1]](#fig_ijdvl_2013_79_4_555_113116_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2013_79_4_555_113116_f2.jpg){kind=link}