Translate this page into:
Interstitial granulomatous dermatitis due to borreliosis
2 Institute of Dermatology, Department of Experimental and Clinical Medicine, University of Udine, Udine, Italy
Correspondence Address:
Nicola di Meo
Institute of Dermatology and Venereology, University of Trieste, Italy Ospedale Maggiore di Trieste, IV Piano Palazzina Infettivi, Piazza Ospedale 1, 34100 Trieste
Italy
| How to cite this article: di Meo N, Stinco G, Trevisan G. Interstitial granulomatous dermatitis due to borreliosis. Indian J Dermatol Venereol Leprol 2015;81:327 |
Sir,
Interstitial granulomatous dermatitis (IGD) is a rare dermatosis of unknown cause with characteristic histopathological features and variable clinical expression. [1] It has been associated with systemic diseases which include rheumatoid arthritis, lupus erythematosus, autoimmune thyroiditis, carcinoma, infections and drug intake. It has recently been proposed that interstitial granulomatous dermatitis could be a cutaneous manifestation of Lyme borreliosis in Borrelia burgdorferi endemic areas. [2],[3],[4] We report a similar case below.
A 63-year-old farmer presented with asymptomatic, asymmetric, erythematous plaques with elevated borders and an annular rope like configuration over his back. The lesions had been progressively enlarging over the last 8 months [Figure - 1]. He also suffered from malaise, non specific myalgia and arthritis since the onset. A punch biopsy specimen taken from a skin lesion showed a normal epidermis and a perivascular and interstitial diffuse infiltrate in the dermis comprising of lymphocytes, histiocytes and a few giant cells without any mucin deposits[Figure - 2]. Palisading granulomas consisting of histiocytes surrounding focally degenerated eosinophilic collagen were also present. The ′floating sign′ was recognizable, which is characterized by histiocytic pseudorosettes that surround an empty space centered by degenerated collagen fibers [Figure - 3]. A diagnosis of interstitial granulomatous dermatitis was made.
 |
| Figure 1: Annular dermatitis depicting the 'Rope sign' |
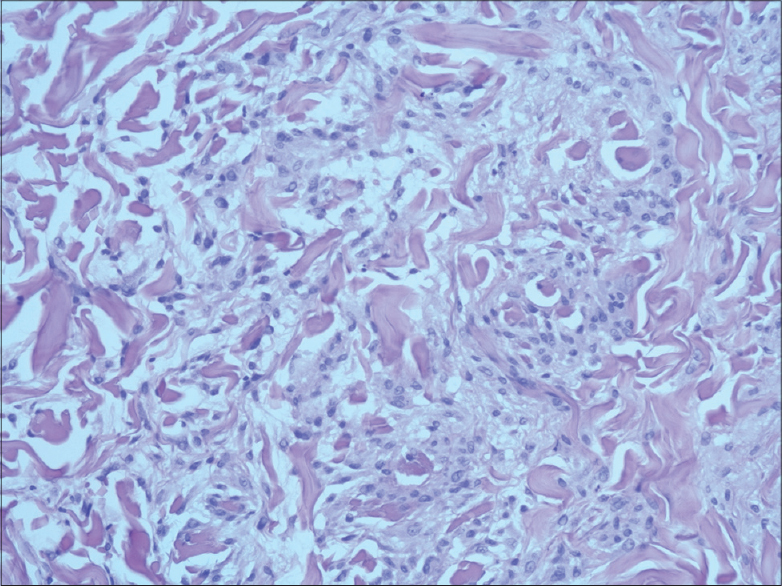 |
| Figure 2: Interstitial diffuse infiltrate of the dermis comprising of lymphocytes, histiocytes and a few giant cells without mucin deposition |
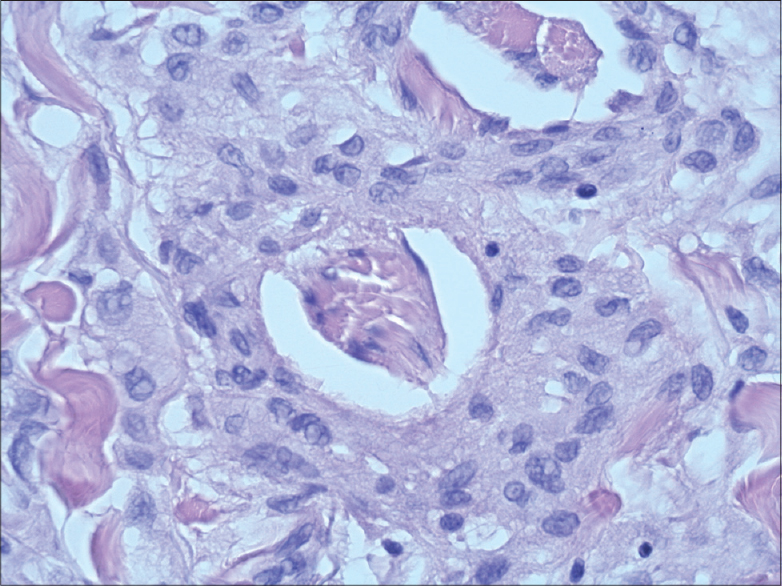 |
| Figure 3: The 'floating sign'. Histiocytic pseudorosettes surrounding an empty space centered by degenerated collagen fibers |
There was no history of drug intake, autoimmune disorders or malignancy. Five months prior to the onset of these lesions, he had developed an erythematous patch over his left thigh one week after a tick bite over the same area. This resulted in a ′bull′s-eye′ appearance which gradually expanded over a period of several days and measured 15 cm across. It spontaneously resolved without any treatment one month later. We performed a two-tiered antibody testing for Lyme disease. High titres of IgG and IgM were detected with the ELISA rapid test (IgG: 233 UA/ml, IgM: 178 UA/ml; normal values:<24 UA/ml) and confirmed by the western blot test. Real time quantitative polymerase chain reaction assays were positive to Borrelia burgdorferi. The patient was treated with doxycycline 200 mg daily for 21 days and hydroxychloroquine 400 mg daily for 4 months with complete resolution of skin lesions and arthromyalgia.
The clinical presentation of interstitial granulomatous dermatitis is quite heterogeneous. Annular patches and non-tender multiple erythematous papules, nodules or plaques on the trunk and proximal extremities are the usual features. Differential diagnoses include all the other conditions that present with erythematous plaques. The presence of cord-like skin lesions (rope sign) is characteristic but is only present in a few patients. [1] Skin lesions are usually asymptomatic or mildly symptomatic. Histopathology reveals an interstitial and palisading granulomatous dermatitis accompanied by piecemeal fragmentation of collagen and elastic fibres. This process is usually accentuated in the reticular dermis but abnormalities can also involve the full thickness of the dermis or hypodermis. The ′floating sign′ has been reported in most published cases. Rare giant multinucleated histiocytes or atypical histiocytes, perivascular and interstitial lymphocytic infiltrates are present in most of the cases described. Epidermal changes, presence of mucin deposits and leukocytoclastic vasculitis are typically absent. [1] Histologically, the main differential diagnoses include interstitial granuloma annulare, palisaded neutrophilic granulomatous dermatitis, granulomatous reactions to drugs, histiocytoid Sweet syndrome and Churg Strauss granulomatosis.
Interstitial granulomatous dermatitis has been reported in association with autoimmune diseases, lymphoproliferative disorders, solid organ cancers and several systemic drugs. In the last decade, Borrelia burgdorferi has been identified in some cases. [2],[3],[4] These usually appeared in the intermediate stage of Lyme disease (between erythema migrans and acrodermatitis chronica atrophicans). It is important to note that the clinical features of the reported cases were similar to those of morphea, erythema migrans and granuloma annulare. [2],[3],[4] In our case, the lesions had features more typical for interstitial granulomatous dermatitis. The mechanism of this association is unknown but it can be assumed that Borrelia antigens persist in different skin sites, stimulating a granulomatous reaction.
In conclusion, interstitial granulomatous dermatitis due to Borrelia burgdorferi infection is certainly a rare clinical manifestation. Recognizing this entity is only achieved through a combined of clinical, histological and molecular approach. It is important to consider this association, especially in endemic areas, in order to provide adequate treatment.
| 1. |
Peroni A, Colato C, Schena D, Gisondi P, Girolomoni G. Interstitial granulomatous dermatitis: A distinct entity with characteristic histological and clinical pattern. Br J Dermatol 2012;166:775-83.
[Google Scholar]
|
| 2. |
Moreno C, Kutzner H, Palmedo G, Goerttler E, Carrasco L, Requena L. Interstitial granulomatous dermatitis with histiocytic pseudorosettes: A new histopathologic pattern in cutaneous borreliosis. Detection of Borrelia burgdorferi DNA sequences by a highly sensitive PCR-ELISA. J Am Acad Dermatol 2003;48:376-84.
[Google Scholar]
|
| 3. |
Gualco F, Zaccaria E, Drago F, Rebora A. Interstitial granuloma annulare and borreliosis: A new case. J Eur Acad Dermatol Venereol 2007;21:1117-8.
[Google Scholar]
|
| 4. |
Fernandez-Flores A, Ruzic-Sabljic E. Granuloma annulare displaying pseudorosettes in Borelia infection. Acta Dermatovenerol Alp Panonica Adriat 2008;17:171-6.
[Google Scholar]
|
Fulltext Views
2,615
PDF downloads
947





![[Figure - 1]](#fig_ijdvl_2015_81_3_327_154783_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2015_81_3_327_154783_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2015_81_3_327_154783_f3.jpg){kind=link}