
Translate this page into:
Intradermal naevus with fat: A distinct variant
Corresponding author: Dr. Sujay Khandpur, Department of Dermatology and Venereology, All India Institute of Medical Sciences, New Delhi, India. sujay_khandpur@yahoo.com
-
Received: ,
Accepted: ,
How to cite this article: Gaurav V, Anand GRP, Khandpur S. Intradermal naevus with fat: A distinct variant. Indian J Dermatol Venereol Leprol. 2025;91:S60-S62. doi: 10.25259/IJDVL_973_2023
Dear Editor,
An intradermal naevus is a common benign melanocytic growth, acquired or congenital, characterised by intradermal clusters of naevus cells.1 These naevi may demonstrate infiltration by adipocytes or lipomatous alterations within naevus cells.2,3 A lobulated intradermal naevus is a distinct variant that clinically presents as a lobulated, yellowish growth with adipocytic infiltration within clusters of naevus cells on histology.2,3 Lipomatous intradermal naevi tend to occur frequently in individuals aged over 50 years. The occurrence of fatty infiltration, fibrosis, neuroid changes, calcification, and ossification likely signifies age-related regression.4 Furthermore, lobulated intradermal naevi are congenital and typically manifest as clusters of growths resembling corymbiform, verrucous or raspberry-like patches or pedunculated nodules.5 Naevi with fat commonly involve the head and neck, especially in women.6
A 21-year-old female presented with a solitary papule on her scalp for 4 years. The lesion was initially noted by her mother while combing the hair. It was asymptomatic at first but gradually grew in size to cause discomfort during combing. Examination revealed a single skin-coloured to yellowish papule, measuring 0.7 × 0.7 cm, located on the vertex of the scalp [Figure 1]. The papule was well-defined, non-tender, non-mobile, and soft to firm. The surrounding skin was unaffected. Polarised dermoscopy revealed a papule with structureless areas along with focal areas showing brown small clods and follicular plug in addition to branched and linear peripheral vessels [Figure 2]. The papule was excised and histologically examined to rule out other appendageal tumours such as adult xanthogranuloma and pilomatricoma. Histology revealed multiple nests of naevoid melanocytes extending from the papillary to the deep reticular dermis in an interstitial pattern and along the hair follicles [Figures 3a and 3b]. Additionally, adipocytes were noted in the superficial and deep dermis [Figure 3c]. Based on the clinical, dermoscopic, and histologic findings, we made a diagnosis of lobulated intradermal naevus of the scalp.

- A solitary skin-coloured to yellowish papule, measuring 0.7 × 0.7 cm, located on the vertex of the scalp.
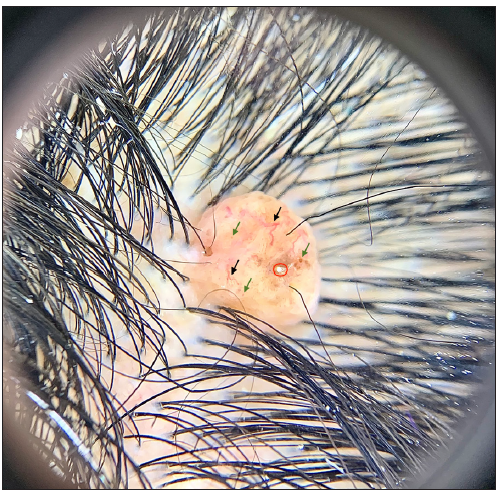
- Polarised dermoscopy showing a papule with structureless areas along with focal areas showing brown small clods (olive green arrows) and follicular plug (red circle) in addition to peripheral linear vessels with branches (black arrows) (Illuco, IDS-1100; 10×).
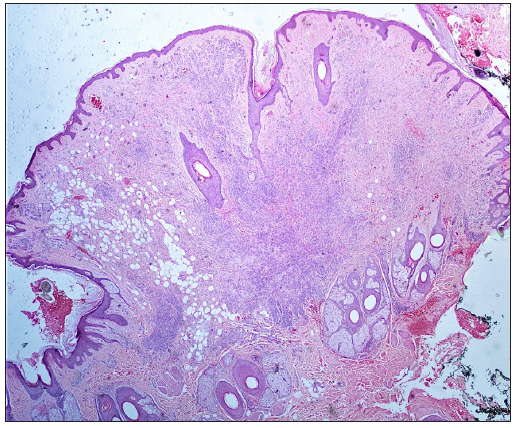
- Histology showing multiple nests of naevoid melanocytes extending from the papillary to the deep reticular dermis and along the hair follicles (Haematoxylin and eosin, 40×).
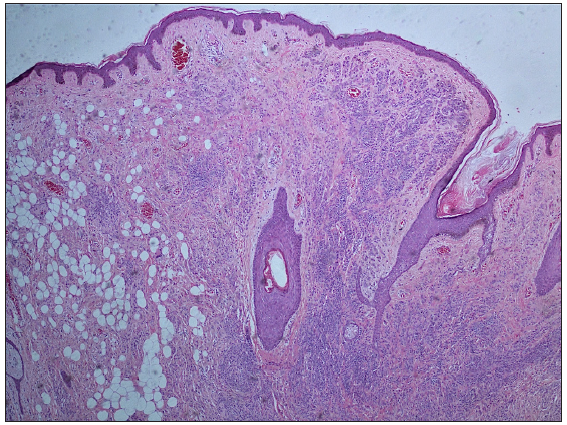
- Congenital growth pattern encircling adnexae and an interstitial growth pattern (Haematoxylin and eosin, 100×).
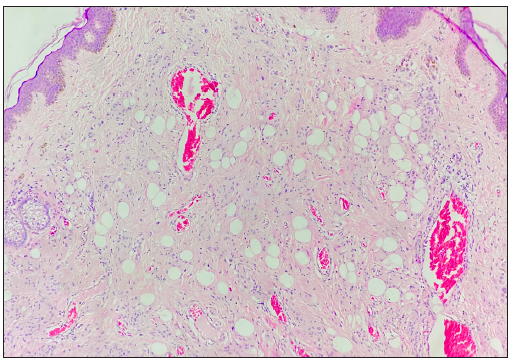
- Adipocytes in the superficial and deep dermis along with naevoid melanocytes (Haematoxylin and eosin, 100×).
Naevi with fat typically presents in young females as a yellowish nodule. This entity is underreported due to its rarity and the potential for misdiagnosis, as it clinically resembles other conditions like naevus lipomatosus superficialis and skin tag.2
Common sites for intradermal naevi include the head and neck region with reports involving the eyelids, oral cavity, external auditory canal, and, gingiva. These lesions are often solitary and can vary in size from a few millimetres to centimetres. Generally, intradermal naevi on the scalp are lobulated and cerebriform.4 However, the present case featured a solitary papule, likely due to earlier presentation than the other reported cases. Acquired intradermal naevi with senescent changes are more common in the elderly which contrasts with the present case.
It is worth noting that in all the previously documented cases in the literature, including the present case, this condition was more frequent in women suggesting a potential link between female gender and lipomatous changes.2,6
The histopathology of congenital melanocytic naevi is essentially identical to that of acquired naevi, except for adnexotropism. Dermal mitotic activity is rare or absent in intradermal naevi. Each acquired intradermal melanocytic naevus can be classified histologically as either Unna’s naevus or Miescher’s naevus. Unna’s naevus primarily involves the adventitial layer, often confined to the expanded papillary dermis and sometimes extending to the perifollicular dermis. Conversely, Miescher’s naevus shows diffuse infiltration of melanocytes into both the reticular dermis and adventitial structures, forming a wedge-shaped pattern.7 Naevus lipomatous superficialis is characterised by the absence of naevus cell nests, presenting instead as clusters or strands of fat cells, often observed on the lower back. In contrast, cerebriform naevus displays solitary or clustered naevus cells with varying melanin content and neuroid transformation but lacks fatty degeneration or fibrosis.2,3
Dermoscopy serves as a non-invasive tool that aids in distinguishing these lesions from other differentials. Among intradermal naevi, the most frequently observed pigment pattern is the brown pigment pattern (37.1%), followed by the cobblestone pattern (30.6%) in Unna’s naevi. For Miescher’s naevi, white areas (23.6%) and a dotted/globule pattern (20%) are characteristic. The most commonly identified vascular pattern is the polymorphic pattern (34.6%) with a combination of comma-shaped and arborising vessels being the prevailing type across all naevi, as reported by Vincenzo Greco et al.8 The yellowish background on dermoscopy, as seen in our case, hints towards lipidisation.
Generally, these lesions tend to persist with rare instances of regression. Surgical excision is usually curative.
In conclusion, we report a rare case of an intradermal naevus with fat in a young female describing the dermoscopic and histologic features to sensitise clinicians about this entity.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
References
- The spectrum of melanocytic nevi and their clinical implications. J Dtsch Dermatol Ges. 2022;20:483-504.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Lobulated intradermal nevus: A rare entity. Indian J Dermatopathol Diagn Dermatol. 2014;1:83-5.
- [CrossRef] [Google Scholar]
- Lobulated intradermal nevus. Report of three cases. J Am Acad Dermatol. 1991;24:74-7.
- [CrossRef] [PubMed] [Google Scholar]
- Age-related changes in melanocytic naevi. Clin Exp Dermatol. 1979;4:49-58.
- [CrossRef] [PubMed] [Google Scholar]
- Four cases of lobulated intradermal nevus: a sign of aging melanocytic nevus. Ann Dermatol. 2011;23:115-8.
- [CrossRef] [PubMed] [Google Scholar]
- Nevus with fat: Clinical characteristics of 100 nevi containing mature adipose cells. J Am Acad Dermatol. 1998;39:704-11.
- [CrossRef] [PubMed] [Google Scholar]
- Unna’s and Miescher’s nevi: Two different types of intradermal nevus: hypothesis concerning their histogenesis. Am J Dermatopathol. 2007;29:141-51.
- [CrossRef] [PubMed] [Google Scholar]
- Dermoscopic patterns of intradermal naevi. Australas J Dermatol. 2020;61:337-41.
- [CrossRef] [PubMed] [Google Scholar]




