Translate this page into:
Intradermal tests in dermatology-II: Tests for noninfectious diseases
Correspondence Address:
Uday Khopkar
Department of Dermatology, Seth GS Medical College and KEM Hospital, Parel, Mumbai - 12
India
| How to cite this article: Pande S, Nagar R, Khopkar U. Intradermal tests in dermatology-II: Tests for noninfectious diseases. Indian J Dermatol Venereol Leprol 2007;73:57-59 |
Introduction
Intradermal tests are widely used to support the diagnosis of dermatological and nondermatological diseases. They are mainly indicated for the detection of immediate (Type I hypersensitivity) and delayed type hypersensitivity (DTH, Type IV hypersensitivity) towards exogenous or endogenous antigens. Intradermal tests for the diagnosis of noninfectious diseases and of other uses in dermatology are discussed in this section.
Before undertaking an intradermal test, it is advisable to stop or avoid systemic steroids, immunosuppressive agents at least three days before the procedure and antihistamines at least seven days prior to the test.
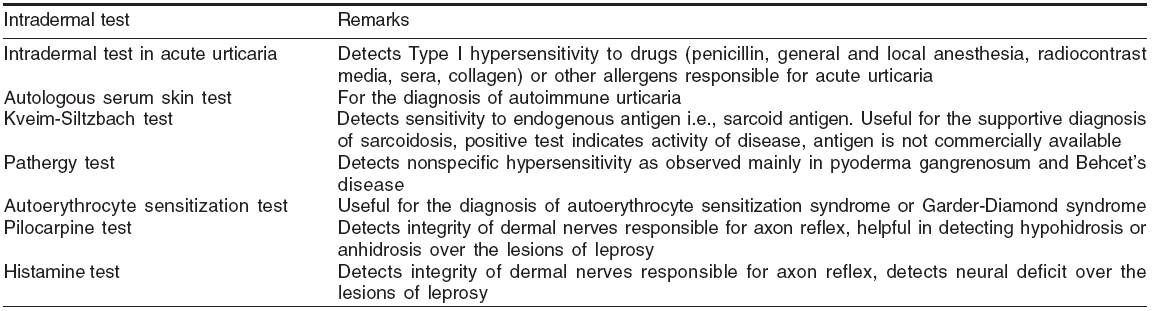
Types of intradermal test for the diagnosis of noninfectious diseases are described in [Table - 1].
Intradermal sensitivity test for common allergens
In cases of acute urinary, intradermal antigens can be used to detect immediate hypersensitivity. Sensitivity to different agents can be identified by using preformed purified antigens, which are commercially available.
Different antigens can be checked at the same time, positive (histamine solution) and negative control (normal saline) are applied for the comparison. Reading is taken 20-30 min following intradermal injection. Alternatively, similar antigens can also be applied on to the skin surface and skin prick testing (SPT) can be performed. Common allergens that are tested in skin prick test are food, fungi, epthelia, pollens and mites. Intradermal tests can be done for similar indications but is rarely advocated as there is more risk and they do not offer added advantages for the prediction of hypersensitivity.
Intradermal sensitivity test for drug[1],[2],[3]
Intradermal testing is a rapid, convenient and reproducible method of detecting drug hypersensitivity (drug-specific IgE antibodies). It is commonly performed for penicillin, general and local anesthetic agents, tetanus toxoid, iodinated radiocontrast media, insulin, heterologous sera, collagen chymopapain etc.
Intradermal testing is in general safe with few reactions and does not appear to result in sensitization. However, resuscitative measures and epinephrine injections should be kept ready as there remains possibility of anaphylaxis.
Penicillin intradermal skin tests should be carried out using major determinant (benzylpenicilloyl polylysine, PPL) and minor determinant mixture (benzyl penicillin, benzyl penicilloate and benzyl penilloate) antigens, these are commercially available. The test can also be performed using 2-10 units of fresh penicillin. Negative intradermal test does not rule out penicillin sensitivity. Other agents are tested similarly for detection of immediate and delayed type of hypersensitivity.
Intradermal skin tests have no predictive value in nonIgE-mediated reactions such as serum sickness, hemolytic anemia, drug fever, interstitial nephritis, contact dermatitis, maculopapular exanthemata or exfoliative dermatitis. Skin testing is contraindicated where there is a history of exfoliative dermatitis, Stevens-Johnson syndrome or TEN.
Predictive sensitization tests[4]
Sensitization index is the relative capacity of a given agent to induce sensitization in a group of humans or animals. Predictive sensitization tests are used to compare the sensitizing properties of new products or chemicals with those of known substances. Both in guinea-pigs and humans, an estimate of the sensitizing potential can be performed using intradermal route. Draize test and Freund′s complete adjuvant test are intradermal methods of testing sensitization potential.
Autologus serum skin testing (ASST)[5],[6],[7]
About 25-45% of patients of chronic idiopathic urticaria have autoantibodies against the high affinity IgE receptor FceRI or IgE that are capable of histamine release. These antibodies, if present in serum, can cause wheal and erythema following intradermal serum injection. This reaction forms the basis of the ASST.
The test is performed by injecting 0.05 ml of the patient′s own serum intradermally into the left flexor forearm two inches below the antecubital crease and a saline control into the right forearm. The optimum combined sensitivity and specificity of the ASST was obtained if a positive test is accepted as a red wheal with a diameter of ³ 1.5 mm than control. Serum is obtained after withdrawing 5 ml of venous blood and standing for about 45 min for separation. The process can be hastened up by centrifugation of the blood.
The cases of idiopathic urticaria which are ASST positive are designated as autoimmune urticaria.
Kveim-Siltzbach test[8],[9],[10]
It is a valuable intradermal test for the diagnosis of sarcoidosis. The test can be utilized to differentiate from other causes of diffuse pulmonary mottling, uveitis and erythema nodosum.
The antigen is prepared from the splenic tissue obtained from a proven case of sarcoidosis either after splenectomy or during autopsy.
About 0.1-0.15 ml of this antigen is injected intradermally, a nodule develops after four to six weeks, which can be biopsied for histopathological confirmation of the diagnosis. False positive reactions were found in an appreciable proportion of patients with Crohn′s disease, ulcerative colitis and tuberculous lymphadenitis, but only with few batches of commercially available antigens.
Pathergy test[11],[12],[13],[14],[15]
Pathergy is the development of a papulopustular lesion around a puncture site on the skin, 24-48h after the injection of a sterile substance like normal saline intradermally. This phenomenon forms the basis of the pathergy test. The test is used as a diagnostic criterion for Behηet′s disease.
Results of the test depend upon the type of needle used; reactivity varies with the diameter and sharpness of needle. The sensitivity and intensity of the reaction is considerably less with sharp needles and needles with smaller diameter.
Pathergy is also a reported phenomenon in pyoderma gangrenosum, in hairy cell leukemia, Hodgkin′s lymphoma and in chronic myeloid leukemia treated with interferon alpha.
Histopathological evaluation of the test is not found to be more sensitive than the clinical evaluation.
Autoerythrocyte sensitization test
The intradermal test for the diagnosis of autoerythrocyte sensitization syndrome is done with washed RBCs of the patient in the intrascapular region with a saline control on the opposite side.[16] Patient develops a painful ecchymotic reaction within two hours at the site of the injection indicating positive test. The control site does not show reaction.
Histamine test[17]
When histamine is injected intradermally, it causes bright red histamine flare due to capillary vasodilatation. However, this effect is due to axon reflex within dermal nerves. Thus the histamine test can be used to test integrity of dermal nerves in cases of tuberculoid leprosy. One drop of histamine acid diphosphate 1 in 1000 (1 mg/ml) is placed on the skin surface. Superficial prick is made through the drop and bright flare will appear within a minute if dermal nerves are intact. Response takes little longer on the extremities.
Pilocarpine test[17]
Similar to the histamine test, the pilocarpine intradermal test is used to detect the integrity of dermal nerves in suspected cases of tuberculoid leprosy. About 0.2 ml of 1 in 1000 solution of pilocarpine nitrate is injected intradermally into the lesion, the injection site is then painted with tincture of iodine and then dusted with starch powder. Sweating, if present, causes blue discoloration of the powder. Alternatively, quinizarin powder can be used in place of starch powder with the advantage that there is no need for painting the test site with tincture of iodine.
| 1. |
Weber EA, Knight A. Testing for allergy to antibiotics. Semin Dermatol 1989;8:204-12.
[Google Scholar]
|
| 2. |
Adkinson NF Jr. Tests for immunoglobulin drug reactions. In : Rose NF, Friedman H, editors. Manual of Clinical Immunology. American Society for Microbiology: Washington DC; 1986. p. 692-7.
[Google Scholar]
|
| 3. |
Shepherd G, Mendelson L. The role of skin testing for penicillin allergy. Arch Intern Med 1992;152:2505.
[Google Scholar]
|
| 4. |
Klezac G. The Freund's complete antigen and open epicutaneous test. A complementary test procedure for realistic assessment of allergenic potential. Curr Probl Dermatol 1986;15:152-71.
[Google Scholar]
|
| 5. |
Sabroe RA, Grattan CE, Francis DM, Barr RM, Kobza Black A, Greaves MW. The autologous serum skin test: A screening test for autoantibodies in chronic idiopathic urticaria. Br J Dermatol 1999;140:446-52.
[Google Scholar]
|
| 6. |
Grattan CE, Francis DM, Hide M, Greaves MW. Detection of circulating histamine releasing autoantibodies with functional properties of anti-IgE in chronic urticaria. Clin Exp Allergy 1991;21:695-704.
[Google Scholar]
|
| 7. |
Godse KV. Autologous serum skin test in chronic idiopathic urticaria. Indian J Dermatol Venereol Leprol 2004;70:283-4
[Google Scholar]
|
| 8. |
Mana J, Pujol R, Salazar A, Morera J, Fite E, Badrinas F. The Kveim-Siltzbach test in sarcoidosis. Med Clin (Barc) 1995;104:645-7.
[Google Scholar]
|
| 9. |
Mitchell DN, Sutherland I, Bradstreet CM, Dighero MW. Validation and standardization of Kveim test suspensions prepared from two human sarcoid spleens. J Clin Pathol 1976;29:203-10.
[Google Scholar]
|
| 10. |
Chase MW. The preperation and standardization of Kveim testing antigen. Amer Rev Resp Dis 1961;84:86-8.
[Google Scholar]
|
| 11. |
Gul A, Esin S, Dilsen N, Konice M, Wigzell H, Biberfeld P. Immunohistology of skin pathergy reaction in Behηet's disease. Br J Dermatol 1995;132:901-7.
[Google Scholar]
|
| 12. |
Criteria for diagnosis of Behcet's disease. International Study Group for Behcet's Disease. Lancet 1990;335:1078-80.
[Google Scholar]
|
| 13. |
Dilsen N, Konice M, Aral O, Ocal L, Inanc M, Gul A. Comparative study of the skin pathergy test with blunt and sharp needles in Behcet's disease: Confirmed specificity but decreased sensitivity with sharp needles. Ann Rheumat Dis 1993;52:823-5.
[Google Scholar]
|
| 14. |
Kaplan RP, Newman G, Saperia D. Pyoderma gangrenosum and hairy cell leukemia. J Dermatol Surg Oncol 1987;13:1029-31.
[Google Scholar]
|
| 15. |
Budak-Alpdogan T, Demircay, Alpdogan O, Direskeneli H, Ergun T, Ozturk A, et al . Skin hyperreactivity of Behcet's patients (pathergy reaction) is also positive in interferon alpha-treated chronic myeloid leukaemia patients, indicating similarly altered neutrophil functions in both disorders. Br J Rheumatol 1998;37:1148-51.
[Google Scholar]
|
| 16. |
Sawhney M, Arora G, Arora S, Prakash J. Undiagnosed purpura: A case of autoerythrocyte sensitization syndrome associated with dermatitis artefacta and pseudo-ainhum. Indian J Dermatol Venereol Leprol 2006;72:379-81.
[Google Scholar]
|
| 17. |
Jopling WH, Mcdougall AC. Diagnostic tests. Handbook of leprosy. 5th ed. CBS Publishers and Distributors: New Delhi; p. 58-66.
[Google Scholar]
|
Fulltext Views
14,459
PDF downloads
6,596





![[Table - 1]](#tbl_ijdvl_2007_73_1_57_30660_1.jpg){kind=link}