Translate this page into:
Kaposi's varicelliform eruption
2 Department of Microbiology, Kasturba Medical College, Light House Hill Road, Mangalore, India
Correspondence Address:
Manjunath M Shenoy
Department of Skin and VD, K. S. Hegde Medical Academy, Deralakatte, Mangalore
India
| How to cite this article: Shenoy MM, Suchitra U. Kaposi's varicelliform eruption. Indian J Dermatol Venereol Leprol 2007;73:65 |
Abstract
Kaposi's varicelliform eruption (eczema herpeticum) is the name given to a distinct cutaneous eruption caused by herpes simplex and certain other viruses that infect persons with preexisting dermatosis. Most commonly it is associated with atopic dermatitis. We report a case of a three-year-old atopic child who presented with extensive vesicular eruption suggestive of Kaposi's varicelliform eruption. There was history of fever, malaise and extensive vesicular eruptions. Diagnosis was made based on clinical features and Tzanck smear examination. Patient responded adequately to oral acyclovir therapy.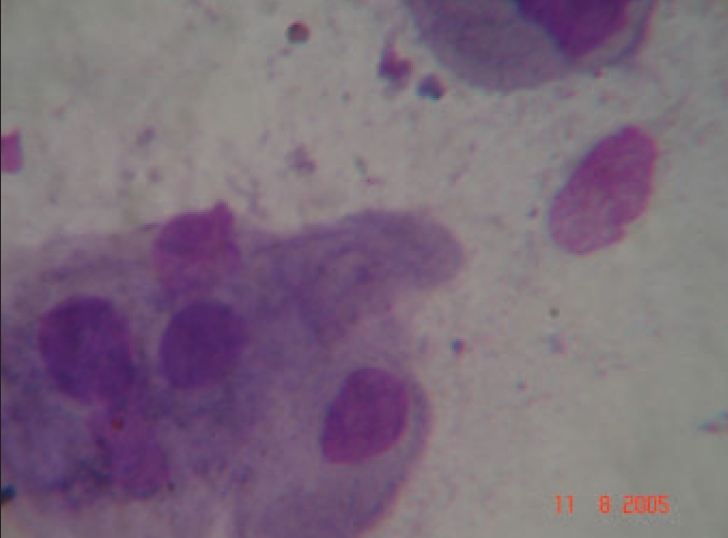 |
| Acantholytic cells and multinucleated giant cell (Leishman stain, x1000) |
|
| Acantholytic cells and multinucleated giant cell (Leishman stain, x1000) |
 |
| Umbilicated vesicles on gluteal and perianal region |
|
| Umbilicated vesicles on gluteal and perianal region |
 |
| Grouped vesicular lesions on posterior neck and upper back |
|
| Grouped vesicular lesions on posterior neck and upper back |
 |
| Grouped vesicular lesions on upper chest |
|
| Grouped vesicular lesions on upper chest |
Kaposi′s varicelliform eruption is a disseminated cutaneous infection caused usually by herpes simplex virus (HSV) occurring in patients with preexisting active dermatitis. Most commonly it is seen in patients with atopic dermatitis; for this reason it is also referred to as eczema herpeticum. It is common during the second to third decade of life.[1] The eruption is mostly disseminated in the areas of dermatitis, with a predilection for the upper body and the head. It is a rare condition and the severity varies from mild transient disease to a fulminating fatal disorder involving the visceral organs. Invariably, onset of symptoms is abrupt, and clusters of umbilicated vesicles appear in areas of abnormal skin. A Tzanck smear from a ruptured vesicle provides rapid diagnosis, however, viral culture of fresh vesicular fluid is the confirmatory test. Treatment with acyclovir shows a good response.
Case report
A three-year-old girl, with a known history of bronchial asthma and atopic dermatitis presented with fever, malaise, generalized itching and occurrence of skin eruptions for the past two days. The patient was on oral bronchodilator and topical emollient since last few months. There was past history of recurrent respiratory tract infections and flairs of dermatitis, which were treated as required. When examined she was febrile (100.4o F) and there were extensive grouped vesicular lesions, many of which were umbilicated. Lesions were distributed on the forehead, cheeks, posterior neck, upper chest, upper back, and perianal and gluteal regions [Figure - 1],[Figure - 2],[Figure - 3]. Generalized dry skin and areas of chronic eczematous lesions over the face, chest, wrists, elbows, back, legs and ankles were also seen. With these features a provisional diagnosis of atopic dermatitis with eczema herpeticum (Kaposi′s varicelliform eruption) was made.
Blood counts revealed leukocytosis (TLC-13,800 cells\ cu. mm) with neutrophilia (78%) and an elevated ESR (36 mm at the end of one hour). Scraping from the blisters and staining (Tzanck smear) showed multinucleated giant cells and acantholytic cells [Figure - 4]. Viral culture was not done due to unavailability of a center doing the test in our locality. However, the classical clinical features along with Tzanck smear findings were confirmative of eczema herpeticum.
Patient was treated with acyclovir suspension (20 mg/kg thrice daily), cefadroxyl syrup (15 mg/ kg body weight 12-hourly), and antipyretics. She improved with the treatment and the skin lesions cleared completely by the eighth day.
Discussion
Kaposi′s varicelliform eruption (eczema herpeticum) is the name given to a distinct cutaneous eruption caused by some viruses but most often by herpes simplex in a patient with a preexisting dermatosis like atopic eczema. Other viruses implicated are Coxsackie′s virus A16 and vaccinia virus. These infections, which otherwise are mild and localized, present in a florid and disseminated manner on the background of such dermatosis due to some unknown reasons. Eczema herpeticum is seen with increasing frequency in adults and it should be considered in the differential diagnosis of vesicular skin lesions occurring in atopic patients.[2] The severity appears to be unrelated to the extent of eczematous lesions, and active dermatitis is not necessary for the development of recurrent eczema herpeticum.[2] Transmission occurs through contact with infected person or by dissemination of primary or recurrent herpes.[3] Recurrent episodes may also occur but are milder and usually not associated with systemic symptoms.[3] The condition is most frequently seen in association with atopic dermatitis but also with mycosis fungoides, pityriasis rubra pilaris, neurodermatitis, irritant contact dermatitis, congenital ichthyosiform erythroderma, ichthyosis vulgaris, pemphigus foliaceus, benign familial pemphigus (Hailey-Hailey disease), Darier disease, Wiskott-Aldrich syndrome, Sezary syndrome, seborrheic dermatitis, skin grafts, burns, cowpox, and rosacea.[3]
It begins as clusters of umbilicated vesiculopustules as in our patient, in areas where the skin had been affected by dermatitis. Tzanck smear can provide rapid diagnosis when it shows the characteristic epithelial multinucleated giant cells and acantholysis. Polymerase chain reaction assays can be used to detect virus; however, virus isolation from vesicular fluid remains the definitive diagnostic approach.[4] Systemic viremia with multiple organs like the liver, lungs, brain, gastrointestinal tract, adrenal glands and eye involvement is the major cause of morbidity and mortality.[3]
It is important to notice how a mild viral infection like herpes simplex gets modified in atopic individuals. T-cell-mediated immunity is important in the control of primary and recurrent HSV infections, and an HSV-specific, cell-mediated immune defect could be the reason for the development of Kaposi varicelliform eruption. A high total serum immunoglobulin E level may also be a risk factor for the development of Kaposi varicelliform eruption.[3] A delay in diagnosis can occur because the eruption may be confused with the underlying disease. A high degree of suspicion, the classical umbilicated vesicles and a positive Tzanck smear led us to an early diagnosis. Presence of multinucleated giant cells in the Tzanck smear is confirmatory of herpes.[1] The early institution of antiviral and antibiotic therapy led to an early and complete recovery.
| 1. |
Gupta N, Augustine M, Jayaseelan E. Eczema herpeticum in two elderly patients. Indian J Dermatol Venereol Leprol 2002;68:306-8.
[Google Scholar]
|
| 2. |
Harindra V, Paffett MC. Recurrent eczema herpeticum: An underrecognised condition. Sex Transm Infect 2001;77:76.
[Google Scholar]
|
| 3. |
Kaposi varicelliform eruption. McKenna J, Krusinski P. [cited on Feb 2006 12]. Available from: www.emedicine.com/derm/topic204.htm.
[Google Scholar]
|
| 4. |
Brooks GF, Butel JS, Morse SA, editors. Herpes viruses. In : Javetz, Melnick, and Adelberg's Medical Microbiology. 22nd ed. Lange Medical Books/McGraw - Hill: New York; 2001. p. 370-90.
[Google Scholar]
|
Fulltext Views
3,121
PDF downloads
1,399





![[Figure - 1]](#fig_ijdvl_2007_73_1_65_30664_1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2007_73_1_65_30664_2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2007_73_1_65_30664_3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2007_73_1_65_30664_4.jpg){kind=link}