Translate this page into:
Large congenital melanocytic nevus with metastatic melanoma with a probable primary in the lung
2 Department of Radiology, Maharajah's Institute of Medical Sciences (MIMS), Nellimarla, Vizianagaram, India
3 Department of Pathology, CARE Hospitals, Hyderabad, India
Correspondence Address:
G Raghurama Rao
Surya Skin Care and Research Center, # 15-1-2, Gopal Sadan, Naoroji Road, Maharanipeta, Visakhapatnam - 530 002, Andhra Pradesh
India
| How to cite this article: Rao G R, Durga Prasad B K, Amareswar A, Vijaya K T, S. Large congenital melanocytic nevus with metastatic melanoma with a probable primary in the lung. Indian J Dermatol Venereol Leprol 2011;77:51-54 |
Abstract
Large congenital melanocytic nevi (>20 cm in greatest diameter) are very rare and are seen in approximately 1 in 20,000 newborns. The major risk these patients face is the development of neurocutaneous melanosis or malignant melanoma. We report a rare case of large congenital melanocytic nevus with metastatic melanoma in a 40-year-old woman. In this case, though the primary was not established with certainty, on the basis of clinical course and radiological evaluation of various organs, we presume that the primary could be in the lung.Introduction
Large congenital melanocytic nevi (LCMN) developed in utero are present in approximately 1 in 20,000 newborns. Apart from cosmetic and psychological sequelae, the greater risk these patients face is the development of neurocutaneous melanosis (NCM) and malignant melanoma (MM). The lifetime risk of melanoma for these patients is 5% or less. [1] We describe a rare case of LCMN with metastatic melanoma with a probable primary in the lung, on the basis of clinical, histological and radiological features.
Case Report
A 40-year-old healthy married woman presented with LCMN (>20 cm in greatest diameter) in the posterior axis of the body involving lower two-thirds of the back, buttocks, lower abdomen and thighs with multiple satellite nevi of varying sizes all over the body [Figure - 1]a. There were no palpable lymph nodes, no organomegaly and no other congenital abnormalities. In the background of LCMN with more than 20 satellite nevi, the case was thoroughly evaluated with all relevant hematological, biochemical, radiological investigations and skin biopsies from three representative sites - one from the center of the LCMN, two from scalp nodules and leg tumors were taken to rule out MM or NCM. Histopathology of these three specimens was consistent with intradermal melanocytic nevus with no evidence of malignancy [Figure - 1]b. All relevant investigations revealed no abnormalities. The patient was counseled and advised to report for follow-up every year. In the first 2 years of follow-up, there was no evidence of NCM or MM. During the third year of follow-up, the patient had sudden convulsion with transient loss of consciousness and was immediately hospitalized. She regained consciousness immediately and was hemodynamically stable without any focal central nervous system deficits. Her Glasgow Coma Scale (GCS) was 15 which denotes that the patient was alert and not in coma. She was thoroughly investigated and all hematological and biochemical tests were normal. Plain computed tomography (CT) brain showed multiple, well-defined hyperdense lesions at the gray white matter junction with moderate perilesional edema. On contrast administration, moderate enhancement of the lesions was noticed. These findings were suggestive of hemorrhagic metastases [Figure - 2]. As MM is one of the causes for producing hemorrhagic metastasis in the brain, an extensive search for the primary was initiated. There were no leptomeningeal lesions. In the background of LCMN, diagnosis of metastatic melanoma was considered. Patient refused for magnetic resonance imaging (MRI) brain. Chest radiograph revealed large, well-defined opacity with lobulated contours in the right para cardiac region [Figure - 3], which is in favor of neoplastic lesion. Contrast CT of the chest revealed mildly enhancing mass lesion in the medial segment of right middle lobe abutting the pleura. Right hilar and carinal lymphadenopathy was also noted [Figure - 4]. No lymphangitis carcinomatosa was seen. There were no focal lesions in the left lung and liver. These findings were suggestive of a primary malignant mass lesion of the lung. CT guided fine needle aspiration cytology (FNAC) smear from the mass lesion in the right lung showed moderately cellular clusters and diffusely scattered large pleomorphic cells. These cells were round to polygonal. Many cells had brownish black pigment in the cytoplasm. Nuclei were hyperchromatic, and few nuclei had prominent one to two nucleoli. Many bare nuclei were seen, background was hemorrhagic and brownish black pigment was seen [Figure - 5]. These features were suggestive of MM. Lung biopsy could not be done due to patient′s non-cooperation. Abdominal ultrasound, echocardiography, upper and lower GI endoscopy were normal. B-scan of the orbit was normal. High resolution ultrasound of the neck, axilla and inguinal regions was performed and no lymphadenopathy was found. Skin biopsies from three representative sites - from the main nevus, scalp and the leg nodules showed features of intradermal nevus with no evidence of malignancy, similar to the previous biopsy reports.
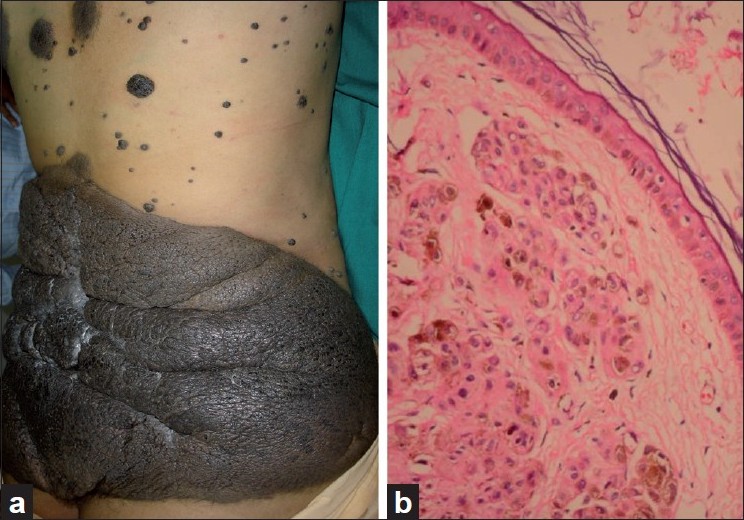 |
| Figure 1 :(a) LCMN on the posterior axis with multiple satellite nevi; (b) nests of nevus cells with no junctional activity (H and E, × x 100) |
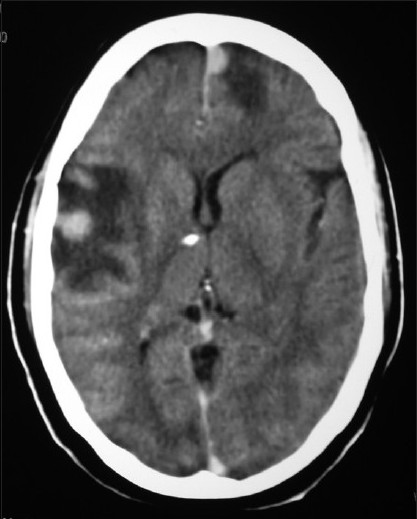 |
| Figure 2 :Contrast CT brain with multiple hemorrhagic metastases – right temporal and left frontal regions |
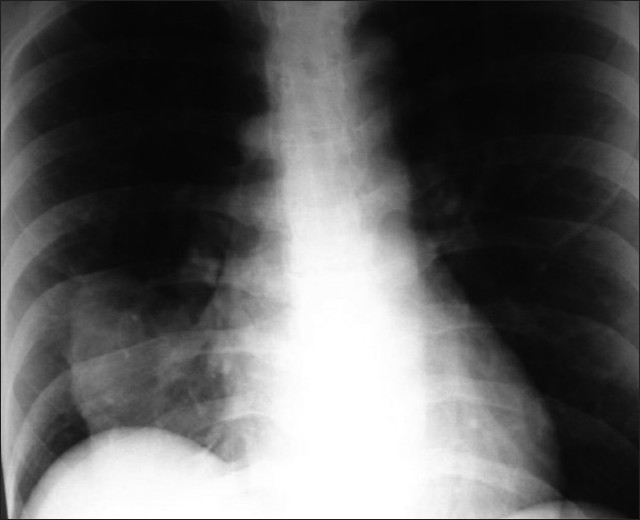 |
| Figure 3 :Chest radiograph showing mass lesion in the right lung |
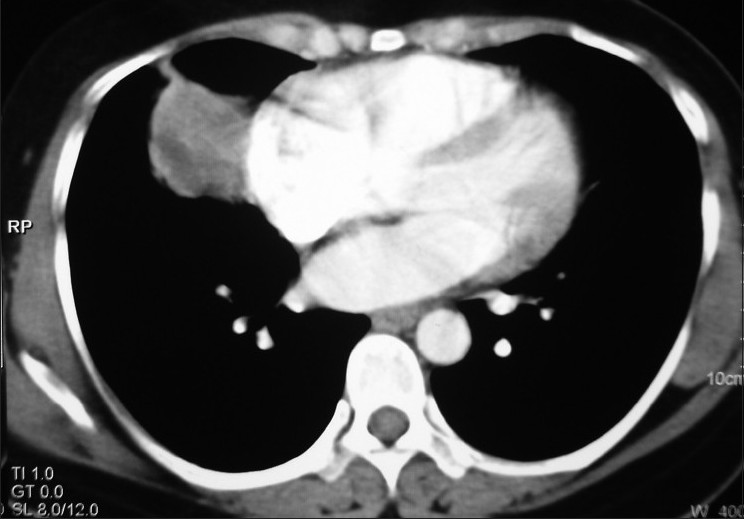 |
| Figure 4 :Contrast CT chest showing mass lesion in the medial segment of right middle lobe |
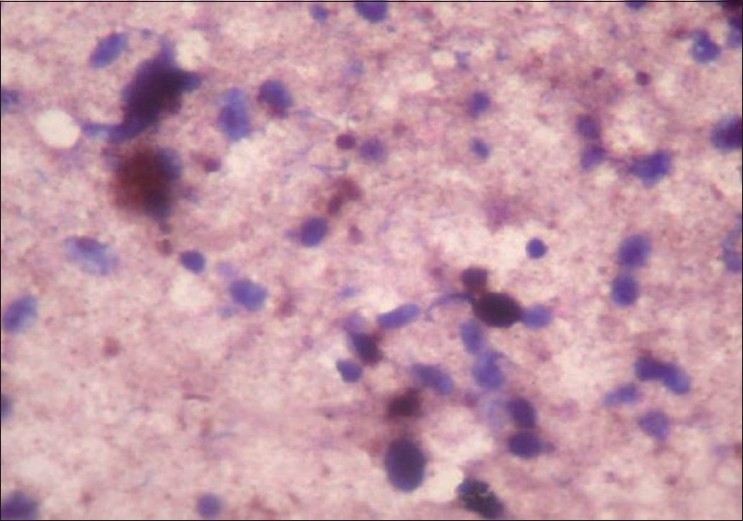 |
| Figure 5 :CT guided FNAC showing scattered large pleomorphic cells with brownish black pigment in the cytoplasm (H and E, ×40) |
During the period of 1 week of hospitalization, the patient′s condition was stable and she was referred to an oncologist for further management. She was given three cycles of Whole Brain Radiation Therapy (WBRT), oral Temozolamide 250 mg daily for 5 days cycle once in 21 days. Follow-up CT scan of the brain after 3 months showed no increase in the size of the metastases, whereas contrast CT of the chest revealed increase in the size of the lung lesion, hilar and carinal lymph nodes. A small hypodense lesion was noticed in the right lobe of the liver which was not previously seen, suggestive of metastasis. There were no neurological complications during her entire illness. She subsequently developed massive malignant right pleural effusion and died.
Discussion
Though the association between LCMN and MM has been established beyond any doubt, the exact magnitude of the risk is still unknown. The lifetime risk of melanoma in these patients has been reported to range from 5 to 40%. [1] In a study of 289 patients with LCMN, 34 patients (12%) developed primary cutaneous melanoma within their nevi, 2 patients had cutaneous maglinant melanoma outside LCMN, 21 patients developed MMs in the central nervous system and 10 had metastatic MM with occult primary. This study further revealed that the development of MMs was more common in axial LCMN than those of the extremities. [2] In another recent review, Hale et al.[3] reported that four of 170 (2.3%) patients developed melanomas, representing a standardized morbidity ratio of 324. They also observed that increasing numbers of satellite nevi and larger LCMN diameters were associated with melanoma and NCM. Another recent study based on a database of 1008 LCMN patients found a significantly lower risk than in previous publications. [4] Chan et al. [5] reported that the risk of melanoma development in LCMN within a predominantly South Asian cohort was very low. To our knowledge, there is no single report of LCMN with MM in the Indian literature.
Metastatic melanoma with an unknown primary is rare and the incidence has been reported to be between 2 and 5%. [6] It is estimated that 70% of melanomas in LCMN developed before the age of 10 years, whereas in our case, MMs developed after 41 years, which is an uncommon feature of LCMN. Multiplicity of lesions and the absence of leptomeningeal involvement ruled out the possibility of primary MM of the brain. These lesions were suggestive of metastases in the brain. The commonest origin of such metastatic lesions in the brain is primary in the lung. Though the primary was not detected with certainty, we presume that there are two possibilities in this case. The primary might be lurking deep in the giant nevus, but repeated skin biopsies from three different sites failed to reveal any evidence of primary melanoma either in the main nevus or in the satellite nevi. Therefore, primary cutaneous melanoma arising from the nevus was ruled out. The other possibility of primary in the lung was considered on the basis of the following radiological findings:
- progressively enlarging solitary lung mass in the right middle lobe,
- progressively enlarging draining lymph nodes,
- no lymphangitis carcinomatosa,
- no other focal lesions in the rest of the lung fields during the entire course of the illness,
- CT guided FNAC from the lung mass revealed MM and
- multiple metastatic lesions in the brain.
In addition, the radiograph of the chest taken just before her death showed a massive right pleural effusion without any focal lesions in the left lung, strongly favoring the diagnosis of primary in the lung rather than metastases. However, the molecular studies of the lung specimens would have been helpful to confirm our clinical suspicion of primary MM of the lung in this case. Primary MM of the lung is a very rare neoplasm, accounting for 0.01% of all lung tumors. In 30% of the cases, primary MM of the lung is an incidental finding on chest radiography. [7] To the best of our knowledge, cases of primary MM of the lung with LCMN background are not found in the literature and hence this interesting rare case is presented. Dermatologists play a vital role in understanding the behavior of all melanocytic nevi including clinical, histological and prognostic aspects, and they also impart the essential health education to the patients. Thus, the dermatologists form the core group along with molecular biologists, pathologists and oncologists to study and evaluate nevi.
| 1. |
Tannous ZS, Mihm MC, Sober AJ, Duncan LM. Congenital melanocytic nevi: Clinical and histopathologic features, risk of melanoma, and clinical management. J Am Acad Dermatol 2005;52:197-203.
[Google Scholar]
|
| 2. |
DeDavid M, Orlow SJ, Provost N, Marghoob AA, Rao BK, Huang CL, et al. A study of large congenital melanocytic nevi and associated malignant melanomas: Review of cases in the New York University Registry and the world literature. J Am Acad Dermatol 1997;36:409-16.
[Google Scholar]
|
| 3. |
Hale EK, Stein J, Ben-Porat L, Panageas KS, Eichenbaum MS, Marghoob AA, et al. Association of melanoma and neurocutaneous melanocytosis with large congenital melanocytic naevi- results from the NYU-LCMN registry. Br J Dermatol 2005;152:512-7.
[Google Scholar]
|
| 4. |
Bett BJ. Large or multiple congenital melanocytic nevi: Occurrence of neurocutaneous melanocytosis in 1008 persons. J Am Acad Dermatol 2006;54:767-77.
[Google Scholar]
|
| 5. |
Chan YC, Giam YC. A retrospective cohort study of Southeast Asian patients with large congenital melanocytic nevi and the risk of melanoma development. J Am Acad Dermatol 2006;54:778-82.
[Google Scholar]
|
| 6. |
Paek SC, Sober AJ, Tsao H, Mihm MC Jr, Johnson TM. Cutaneous melanoma. In: Wolff K, Goldsmith LA, Katz SI, Gilchrest BA, Paller AS, Leffell DJ, editors. Fitzpatrick′s Dermatology in General Medicine. 7 th ed. New York: Mc Graw Hill Companies Inc; 2008. p. 1134-57.
[Google Scholar]
|
| 7. |
Apostolos Dountsis, Charalambos Zisis, Evangelia Karagianni and Jubrail Dahabreh. Primary Malignant Melanoma of the Lung: A Case Report. World Journal of Surgical Oncology 2003;1:26. Available from: http://www.wjso.com/content/1/1/26 [last accessed on 2010 Mar 2].
[Google Scholar]
|
Fulltext Views
3,444
PDF downloads
3,646





![[Figure - 1]](#fig_ijdvl_2011_77_1_51_74980_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2011_77_1_51_74980_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2011_77_1_51_74980_f3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2011_77_1_51_74980_f4.jpg){kind=link}
![[Figure - 5]](#fig_ijdvl_2011_77_1_51_74980_f5.jpg){kind=link}