
Translate this page into:
Large plaque-type blue naevus with subcutaneous cellular nodules (LPTBN-SN) in a young female: A rare entity

Corresponding author: Dr. Keshavamurthy Vinay, Department of Dermatology, Venereology and Leprology, Postgraduate Institute of Medical Education and Research, Chandigarh, India. vinay.keshavmurthy@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Sharma A, Bishnoi A, Chatterjee D, Vinay K. Large plaque-type blue naevus with subcutaneous cellular nodules (LPTBN-SN) in a young female: A rare entity. Indian J Dermatol Venereol Leprol. 2025;91:393-5. doi: 10.25259/IJDVL_1192_2023
Dear Editor,
A 25-year-old woman presented with an asymptomatic, well to ill-defined, raised bluish plaque with superimposed papulo-nodular lesions imparting a cobblestoned appearance covering the right side of the face below the eye [Figure 1]. The lesion had been present since birth but had slowly progressed over the years with relatively faster expansion and new onset neck swellings since the past year. There was enlargement of the submental, submandibular, jugular, retro-auricular and supraclavicular groups of lymph nodes on the same side. The largest of these was the retro-auricular lymph node (4 × 2 cm). Local site ultrasonography showed iso- to hyperechoic soft tissue thickening in the subcutaneous plane with small rounded hypoechoic nodules. Magnetic resonance imaging showed thickening of the dermis and epidermis in the right temporomandibular region with cervical lymphadenopathy suspicious of a malignant transformation. Positron emitted tomography (PET) scan showed increased uptake in the right supraclavicular, axillary, and submental, submandibular, upper, and middle jugular lymph nodes.
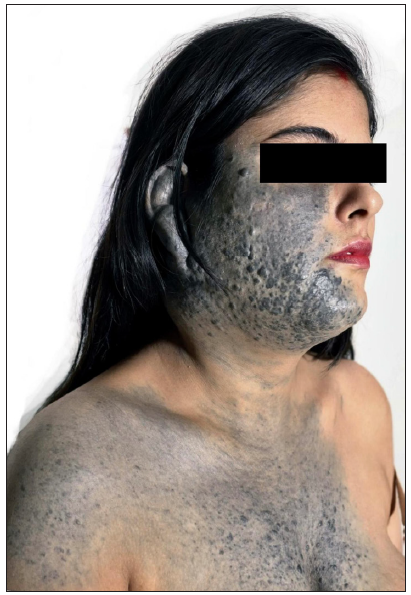
- Presence of a well to ill-defined bluish plaque with superimposed papulo-nodular lesions covering the right side of the face below the eye and extending to involve the ear, retro auricular area posteriorly and the neck and upper chest anteriorly
Ultrasound-guided fine-needle aspiration cytology from right upper cervical swelling yielded smears which were highly cellular and showed aggregates of tumour cells. These tumour cells were mildly pleomorphic with round nuclei, coarse chromatin, tiny nucleoli and moderate amount of cytoplasm with intracytoplasmic melanin pigment identified. Skin biopsy was done with possibilities of malignant melanoma and large plaque-type blue naevus with subcutaneous cellular nodules (LPTBN-SN). Histopathology showed a diffuse pigmented lesion in the dermis [Figure 2a]. The dermis showed melanocytes and pigmented dendritic cells in a background of thick collagen bundles; however, abnormal mitosis or necrosis was not identified [Figure 2b]. Overall, the features were consistent with blue naevus (BN). Lymph node core biopsies showed tumour cells arranged in nests and sheeting patterns [Figure 2c]. High power examination showed naevus cells with mild nuclear atypia, some cells showed intracytoplasmic melanin but no mitosis/necrosis [Figure 2d]. Immunohistochemistry showed positive staining with melanocytic markers of SOX10, S-100, and Melan-A; however, the Ki67 study revealed a low proliferation rate. Subsequently, PReferentially expressed Antigen in MElanoma (PRAME) also came out negative in both skin and lymph node biopsies. After plastic surgery and otorhinolaryngology opinions, a plan for debulking the plaque with neck dissection followed by skin grafting was proposed. Over a follow-up of 12 months, no signs or symptoms suggestive of malignant transformation or distant metastasis were observed.

- Skin biopsy from the preauricular and postauricular region showed a diffuse pigmented lesion in the dermis (Haematoxylin and eosin, 40x)

- Dermis showed melanocytes and pigmented dendritic cells in a background of thick collagen bundles (Haematoxylin and eosin, 200x)

- Core biopsy from lymph node showed a cellular tumour (Haematoxylin and eosin, 20x)

- High power showed naevus cells with mild nuclear atypia, some cells showed intracytoplasmic melanin, and no mitosis/necrosis was noted (Haematoxylin and eosin, 200x)
Dermal melanocytoses (DMs) are a diverse group of benign cutaneous lesions characterised by dendritic melanocytes in the dermis. While all varieties have similar histological features, some manifest as papules, nodules, plaques (blue naevus), bluish or grey patches (Mongolian spots, naevus of Ota, etc.), or they may combine all of these into a single lesion (LPTBN-SN). Busam et al. coined the term LPTBN-SN when two cases of an uncommon type of BN were misdiagnosed as malignancy at first [Table 1]. Both cases underwent excision of the lesion with no signs of progression or recurrence after 32 and 19 months, respectively.1 In another case, cellular BN mimicking metastatic melanoma to the breast was reported.2 Histologically, blue naevi are characterised by the presence of dendritic melanocytes located deep within the dermis. These melanocytes are often spindle-shaped and may be arranged in nests or cords. The dermis may show a prominent fibrous stroma as was seen in our case. We thoroughly reviewed the clinical presentation, histopathological findings and ancillary tests to reach the diagnosis.
| Study (n) | Diagnosis | Management (if mentioned) |
|---|---|---|
| Busam et al.1 (n = 2) | Large plaque-type blue naevus with subcutaneous cellular nodules | Complete excision of the lesion and the man underwent only partial excision of the lesion. |
| Hoos et al.2 (n = 1) | Giant cellular blue naevus of the anterior chest wall | Complete excision of the chest wall naevus and modified radical mastectomy |
| North et al.3 (n = 2) | Melanoma ex blue naevus: Melanoma resembling large plaque blue naevus | Not described |
| Skowron et al.5 (n = 1) | Large plaque-type blue naevus with subcutaneous cellular nodules | Not described |
| Hsiao et al.6 (n = 1) | Facial plaque-type blue naevus | Excision of this unusual plaque-type blue naevus with reconstruction using a tissue expander |
| Yeh et al.7 (n = 1) | Melanoma arising in a large plaque-type blue naevus with subcutaneous cellular nodules | Surgical excision of the subcutaneous cellular blue naevus-like nodule |
| Spring et al.8 (n = 1) | Agminated blue naevus of the plaque type | Removal of the superficial part of the mole with adjuvant skin undermining and a total skin graft |
It can be challenging to tell a cellular BN with unusual features apart from a melanoma that resembles a BN.3 Cytological atypia (mild vs. severe), number of mitotic figures (≤3/mm2 vs. >3/mm2), atypical mitotic figures (absent vs. present), necrosis (rare vs. often), ulceration (rare vs. occasional), lymphovascular invasion (absent vs. occasional) and border (usually well circumscribed vs. often infiltrative) are the main differences between atypical BN and BN-like melanoma. The G-protein coupled receptors, GNAQ and GNA11, have been implicated in early melanocytic proliferation, according to molecular research. Somatic GNAQ mutations have been found in malignant BN (50%) and uveal melanoma (46%) as well as BN (83%). BN and its variants relatively seldom have genetic mutations in common genes like BRAF, NRAS or c-kit, unlike common naevi and melanoma.4
Because lymph node deposits in DMs resemble malignant metastases, diagnosis might be difficult. However, the individual morphology of the tumour cells can help in distinguishing the two entities. Although difficult, most studies recommend complete excision of such lesions owing to the high risk of transformation to malignant melanoma.5–8 This however, becomes challenging in cases like ours where the lesion is too large to excise and involves cosmetically crucial areas like the face and vital areas like the neck, calling for a delicate neck dissection. Newer molecular techniques like fluorescence in situ hybridisation (FISH), comparative genomic hybridisation (CGH), or next-generation sequencing (NGS) can help in establishing the diagnosis in challenging cases but have limited availability.
Large blue naevi with a deep, multi-nodular component are often misjudged as malignant melanoma and should be assessed carefully. Melanotic deposits in the regional lymph nodes add to the complexity of this situational conundrum. Understanding the morphology and histopathology improves our understanding of melanocytic tumours on the whole and helps prevent misinterpretation of this entity as malignant melanoma.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
References
- Large plaque-type blue nevus with subcutaneous cellular nodules. Am J Surg Pathol. 2000;24:92-9.
- [CrossRef] [PubMed] [Google Scholar]
- Giant cellular blue nevus of the anterior chest wall mimicking metastatic melanoma to the breast: a case report. J Surg Oncol. 2000;74:278-81.
- [CrossRef] [PubMed] [Google Scholar]
- Melanoma ex blue nevus: Two cases resembling large plaque-type blue nevus with subcutaneous cellular nodules. J Cutan Pathol. 2012;39:1094-9.
- [CrossRef] [PubMed] [Google Scholar]
- Differential diagnosis of heavily pigmented melanocytic lesions: Challenges and diagnostic approach. J Clin Pathol. 2015;68:963-70.
- [CrossRef] [PubMed] [Google Scholar]
- Large plaque-type blue naevus with subcutaneous cellular nodules. Clin Exp Dermatol. 2009;34:e782-4.
- [CrossRef] [PubMed] [Google Scholar]
- Facial plaque-type blue nevus and its reconstruction. Ann Plast Surg. 1995;35:326-9.
- [CrossRef] [PubMed] [Google Scholar]
- Melanoma arising in a large plaque-type blue nevus with subcutaneous cellular nodules. Am J Surg Pathol. 2012;36:1258-63.
- [CrossRef] [PubMed] [Google Scholar]
- Large agminated cellular ‘plaque-type’ blue nevus surrounding the ear: A case and review. Dermatology. 2013;227:21-5.
- [CrossRef] [PubMed] [Google Scholar]




