Translate this page into:
Lasers for treating striae: An emergent need for better evidence
Correspondence Address:
Kabir Sardana
466, Sector 28 Noida, Uttar Pradesh
India
| How to cite this article: Sardana K. Lasers for treating striae: An emergent need for better evidence. Indian J Dermatol Venereol Leprol 2014;80:392-394 |
Striae distensae or stretch marks is a common skin abnormality affecting both sexes and all races. [1] These lesions usually evolve through various stages which are important to appreciate before attempting any intervention. [2],[3] They are considered to be linear dermal scars with epidermal atrophy as evidenced by the fine wrinkled appearance and telangiectasia. In the acute stage, they are red or violaceous and are referred to as striae rubra, while over time they transform into white, atrophied, and depressed scars, referred to as striae alba. [2] Irrespective of the treatment modality, newer lesions respond much better than old lesions. [1],[2] Various lasers have been used to target various components of the lesion but they should demonstrate both clinical improvement in depth and width and histological improvement with increase in the numbers of collagen and elastin fibers. [2]
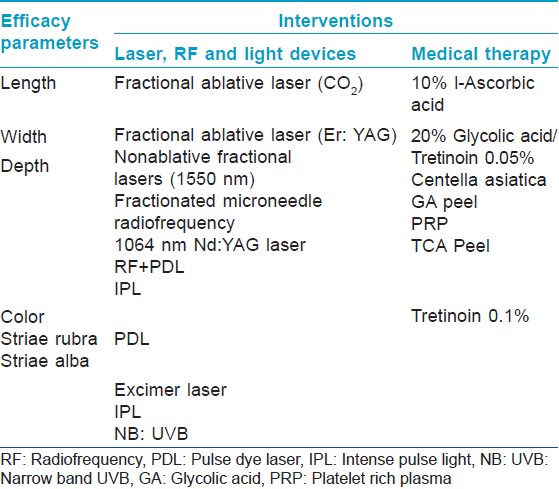
All the available technologies have been used for striae including Er: Glass laser (1550 nm), 1540 nm, fractional Er: YAG/CO 2 and radiofrequency. [3],[4],[5],[6],[7] Of these technologies, the fractional photothermolysis is the most dependable. [2] It creates multiple non-contiguous zones of thermal damage in the epidermis and dermis, sparing the tissue surrounding the wound which in turn stimulates epidermal turnover and dermal collagen remodeling, which results in improvement of a variety of scar types. As all fractional lasers target water which is the primary chromophore they are safe and we prefer using the 1540 nm as it has a relatively lower absorption spectrum for water and thus can produce more collagen remodeling. Since the pathology is in the upper dermis, little difference is expected between non-ablative fractional resurfacing (NAFR) and ablative fractional resurfacing (AFR) as seen in a study in Asian skin (Yang YJ). [7] Though a plethora of devices have been used [Table - 1], the result with most devices has rarely been compared with a placebo group and in my opinion there is a good chance that the patients may have had spontaneous remission.
Striae albae appear pale, depressed and wrinkled and are akin to atrophic scars. The result of lasers for atrophic scars, in general are beset with three problems. Firstly, objective assessment is rarely the norm with percentile scoring and visual analogue scores (VAS) used to assess improvement, which are highly subjective. Moreover, it is impossible to assess three-dimensional improvement by surface evaluation [Figure - 1]. For objective evaluation of skin topography, imaging devices may be used, including three-dimensional (3D) cameras, reflectance confocal microscopy and epiluminescence colorimetry. [8] The second issue is the lack of double-blind trials, even though such studies are difficult to perform with lasers. Having a control group with no treatment or other medical therapies could be a simple method of comparison. It is well known that striae rubra can partially resolve with time and that occasionally striae alba may also do so due to tissue remodeling. [1] This probably explains the results of tretinoin 0.1% which has maximal efficacy in striae rubrae and poor, unpredictable responses in striae albae. [8],[9] Thus, an elegant trial method could be a split lesion or a half side comparison of a laser with a topical agent or placebo. The third issue is demonstration of histological improvement which I believe is the "gold standard" for documenting results. Though this proves merely that the laser has initiated a dermal healing process, but as the results with scars take an average of 6-9 months, this is a good method for documenting results. [7] In a study by Shokeir et al., [10] striae rubra were noted to respond better than striae albae to PDL or IPL as assessed clinically by the width, color, and texture of the striae; however, this difference was not borne out by histological studies! This reiterates the principle that the early scars respond best to most interventions and histology can prove to be the gold standard to validate results.
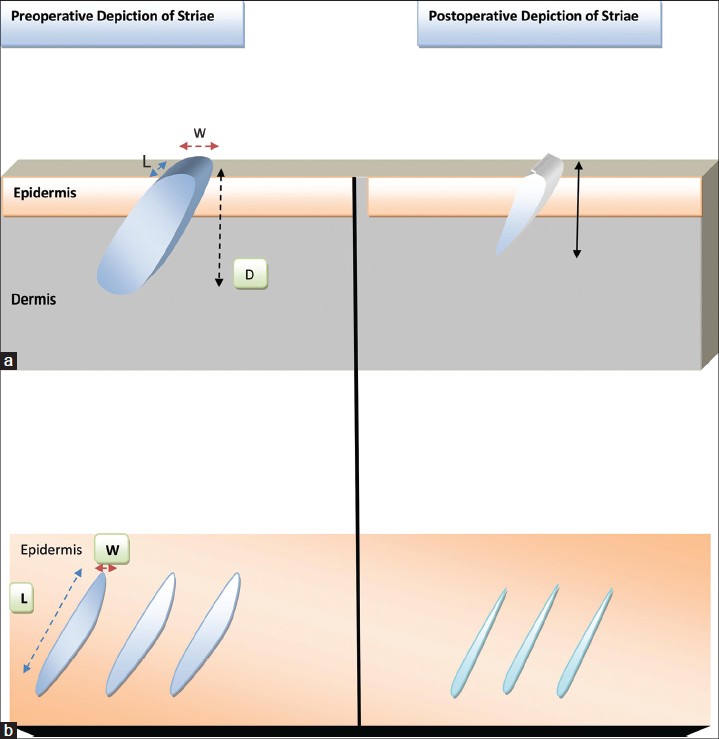 |
| Figure 1: (a) A diagrammatic three-dimensional depiction of Striae distensae, which depicts the pathology akin to an atrophic scar with a depth up to the mid dermis. The laser employed should be able to ameliorate all the dimensions (L: length, W: width and D: depth) of the scar. (b): A surface "topographical" depiction of striae. As striae are linear tissue defects with a length and a width, both need to be addressed in its treatment. The postoperative view depicts a "realistic" partial amelioration of the scar |
When using lasers and light devices, it is important to differentiate between devices that merely work on the "color" and those that actually remodel the scar. Most fractional lasers and RF devices are effective in the treatment of atrophic acne scars, but striae are longer and wider than atrophic acne scars and may not respond completely to laser devices [Figure - 1]. Length and width measurements of striae distensae and histological studies on punch biopsies are rarely reported and these are crucial for assessing the results of treatment.
I am wary of studies that combine more than one method of therapy [6] as there is little way of assessing which therapy ultimately contributes to results. It must also be emphasized that striae have a tendency to resolve spontaneously and crediting lasers with all the improvement noted is probably an injustice to the normal healing response, a fact most authors rarely admit in their manuscripts. An ideal study would be a split lesion comparison of a laser intervention with a medical therapy, with a control group. Objective assessment tools including histology should be used. The study should focus on striae alba and include a post treatment follow up of 6 months. Such a study would be able to arrive at a firm conclusion about the role of lasers in striae.
What should we do for patients who seek treatment for striae? As it is well known that striae tend to become less conspicuous with time, a good practice is to reassure the patient who is not overly concerned about his or her striae. Hermanns and Piérard [8] had described two additional types of striae distensae, striae nigrae and striae caerulea, which occur in darker skin due to increased melanization but very little data exists on these entities, even from India. These striae may merge with the dark skin tones in Indian patients and may not need any treatment. There is data to suggest that medical therapy may be useful in early cases [1] [Table - 1]; tretinoin 0.1%, silicone gels, cocoa butter and Centella asiatica have some data to recommend their use. [9]
In conclusion, as no high-quality, large, double-blind randomized controlled trial in the literature supports the use of creams and laser/light devices in the prevention and treatment of striae distensae and most non-ablative dermal modeling procedures have a risk of post-inflammatory hyperpigmentation in dark skin types, the latter should be used sparingly, if at all for treating striae distensae.
| 1. |
Emer JJ, Khor H. Striae. In: Lebwohl MG, Warren RH, Berth-Hones J, Coulson I, editors. Treatment of skin disease comprehensive therapeutic strategies. 4 th ed. United States: Saunders, Elsevier Limited; 2014. Available from: https://www.expertconsult.inkling.com. [Last accessed on 2014 Jun 14].
[Google Scholar]
|
| 2. |
Sardana K. Lasers for scars, keloids and stretch marks. In: Sardana K, Garg VK, editors. Lasers in Dermatological practice. 1 st ed. New Delhi: Jaypee Brothers; 2014. p. 316-78.
[Google Scholar]
|
| 3. |
Al-Dhalimi MA, Abo Nasyria AA. A comparative study of the effectiveness of intense pulsed light wavelengths (650 nm vs 590 nm) in the treatment of striae distensae. J Cosmet Laser Ther 2013;15:120-5.
[Google Scholar]
|
| 4. |
Gauglitz GG, Reinholz M, Kaudewitz P, Schauber J, Ruzicka T. Treatment of striae distensae using an ablative Erbium: YAG fractional laser versus a 585-nm pulsed-dye laser. J Cosmet Laser Ther 2014;16:117-9.
[Google Scholar]
|
| 5. |
Jiménez GP, Flores F, Berman B, Gunja-Smith Z. Treatment of striae rubra and striae alba with the 585-nm pulsed-dye laser. Dermatol Surg 2003;29:362-5.
[Google Scholar]
|
| 6. |
Suh DH, Lee SJ, Lee JH, Kim HJ, Shin MK, Song KY. Treatment of striae distensae combined enhanced penetration platelet-rich plasma and ultrasound after plasma fractional radiofrequency. J Cosmet Laser Ther 2012;14:272-6.
[Google Scholar]
|
| 7. |
Yang YJ, Lee GY. Treatment of Striae Distensae with Nonablative Fractional Laser versus Ablative CO (2) Fractional Laser: A Randomized Controlled Trial. Ann Dermatol 2011;23:481-9.
[Google Scholar]
|
| 8. |
Hermanns JF, Pierard GE. High-resolution epiluminescence colorimetry of striae distensae. J Eur Acad Dermatol Venereol 2006;20:282-7.
[Google Scholar]
|
| 9. |
Al-Himdani S, Ud-Din S, Gilmore S, Bayat A. Striae distensae: A comprehensive review and evidence-based evaluation of prophylaxis and treatment. Br J Dermatol 2014;170:527-47.
[Google Scholar]
|
| 10. |
Shokeir H, El Bedewi A, Sayed S, El Khalafawy G. Efficacy of pulsed dye laser versus intense pulsed light in the treatment of striae distensae. Dermatol Surg 2014;40:632-40.
[Google Scholar]
|
Fulltext Views
3,460
PDF downloads
2,082





![[Table - 1]](#tbl_ijdvl_2014_80_5_392_140288_b1.jpg){kind=link}
![[Figure - 1]](#fig_ijdvl_2014_80_5_392_140288_u2.jpg){kind=link}