Translate this page into:
Lichen nitidus presenting with trachyonychia
2 Department of Pathology, Medical Faculty, Namik Kemal University, Tekirdag, Turkey
Correspondence Address:
Hulya Albayrak
Department of Dermatology, Medical Faculty, Namik Kemal University, Tekirdag
Turkey
| How to cite this article: Albayrak H, Yanık ME, Erfan G, Oznur M, Kulac M. Lichen nitidus presenting with trachyonychia. Indian J Dermatol Venereol Leprol 2017;83:516 |
Sir,
Trachyonychia is a rare idiopathic dystrophy characterized by a lack of nail luster, longitudinal striations, distal splitting and excessive ridging.[1] One nail or all may be affected and it may be related to autoimmune diseases such as vitiligo and alopecia areata. Histology also may differ according to the associated diseases. Lichen nitidus is a rare, asymptomatic, cutaneous eruption more prevalent among children and young adults with multiple, skin-colored or erythematous papules of millimetric dimensions. The typical distribution of lesions includes the penis, genital area, abdomen and extremities. Nail and mucosal involvement and palmo-plantar hyperkeratosis are rare clinical presentations of this disease.[2] We found seven previously published cases of lichen nitidus with nail changes but were unable to find any previous reports of lichen nitidus with involvement of all twenty nails.
A 5-year-old boy presented with an asymptomatic eruption and dystrophy of all nails for the last 3 months. He had not taken any medications prior to the onset of the eruption and there was no personal or family history of previous dermatological disease. Physical examination revealed multiple, skin-colored papules of pinhead-size present on the right wrist, dorsum of the right hand, proximal periungual region and right knee [Figure 1a], [Figure 1b] ,[Figure 1c], [Figure 1d]. There were longitudinal striations and distal splitting accompanied by sandpaper appearance and lack of luster on the nails of all the fingers and toes [Figure - 2]. No mucosal involvement was observed. Histopathologically, there was hyperkeratosis and parakeratosis in the epidermis with a well circumscribed, papillary dermal lymphoplasmacytic cellular infiltrate within a few rete ridges biopsy [Figure - 3]. Based on physical examination and histopathological findings, the skin eruption was diagnosed as lichen nitidus. Furthermore, trachyonychia was clinically diagnosed according to the nature of nail involvement of all the fingers and toes which included monomorphic longitudinal striations, sandpaper appearance and lack of luster on the nails. The patient was given topical corticosteroid therapy for his skin lesions. Systemic or intralesional treatment was not given for nail involvement and nail lesions were followed up for four months.
 |
| Figure 1a: Lichen nitidus on the wrist |
 |
| Figure 1b: Lichen nitidus lesions on the knee |
 |
| Figure 1c: Lichen nitidus lesions on the nails |
 |
| Figure 1d: Lichen nitidus lesions on the thumbnails |
 |
| Figure 2: Longitudinal striations and distal splitting on nails of all fingers and toes |
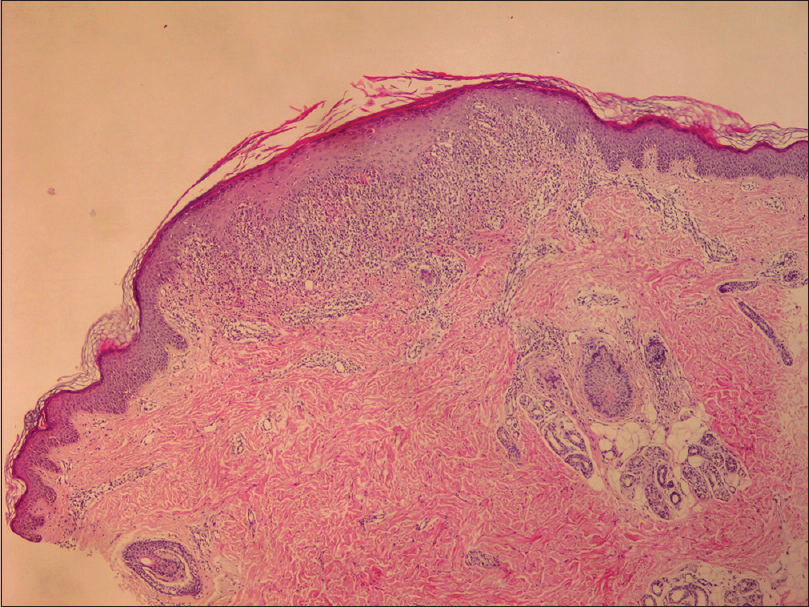 |
| Figure 3: Histological pattern of papule of the knee (H and E, ×400) |
Nail abnormalities are very rare in lichen nitidus.[2],[3],[4] The most characteristic nail lesions are irregular longitudinal grooving and ridging of the nail plate. Nail folds can be normal or have non-specific inflammation.[4] We found seven previous reports of lichen nitidus with nail changes. Of these, four patients had pitting which is a sign of spread of the disease and was absent in our patient.[4] Three cases of lichen nitidus with nail involvement showed symptoms of inflammation such as swelling of periungual tissue and pigmentation of the nail. Furthermore, two of them had lichenoid papules in the periungual area. Lichenoid papules were also present in our case in the nail fold without any signs of inflammation.
Nail changes are mild and restricted in lichen nitidus with the absence of anonychia or pterygium formation.[3] Palmoplantar hyperkeratosis and mucosal involvement are also very rare findings. We found previous reports of three patients with nail involvement who also had palmo-plantar involvement and one of them had oral lesions. On the other hand, our patient had no keratoderma or mucosal lesions. Trachyonychia begins in childhood and affects boys and girls equally.[5] The condition is characterized by longitudinal ridging, alternating elevation and depression, pitting, loss of luster, roughening and sandpaper appearance of the nail surface. It is bilateral and symmetrical. Slight nail abnormalities slowly progress over the years to cause changes in the texture of the nails. Rarely, trachyonychia has been reported to be associated with lichen planus, eczema, psoriasis and alopecia areata, vitiligo, pigment incontinence, alopecia universalis and ichthyosis vulgaris.[1],[5]
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Makkar M, Pandey P, Dixit A, Kapur K, Mahajan NC. Twenty nail dystrophy associated with lichen planus in a child. Iran J Dermatol 2011;14:113-6.
[Google Scholar]
|
| 2. |
Tay EY, Ho MS, Chandran NS, Lee JS, Heng YK. Lichen nitidus presenting with nail changes- case report and review of the literatüre. Pediatr Dermatol 2015;32:386-8.
[Google Scholar]
|
| 3. |
Natarajan S, Dick DC. Lichen nitidus associated with nail changes. Int J Dermatol 1986;25:461-2.
[Google Scholar]
|
| 4. |
Munro CS, Cox NH, Marks JM, Natarajan S. Lichen nitidus presenting as palmoplantar hyperkeratosis and nail dystrophy. Clin Exp Dermatol 1993;18:381-3.
[Google Scholar]
|
| 5. |
Sehgal VN. Twenty nail dystrophy trachyonychia: An overview. J Dermatol 2007;34:361-6.
[Google Scholar]
|
Fulltext Views
3,922
PDF downloads
2,100





![[Figure - 2]](#fig_ijdvl_2017_83_4_516_196316_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2017_83_4_516_196316_f3.jpg){kind=link}